Download
1 / 12
120 likes | 201 Views
BIG ISSUES Survey Results Nicholas Love Hannah Gill. Two week response time 195 people opened the survey 162 people ranked top 4 responses 97 people ranked all 12 14 people gave free text response. Rank-Weighting. A topic that was ranked 1 st got 12 points

E N D
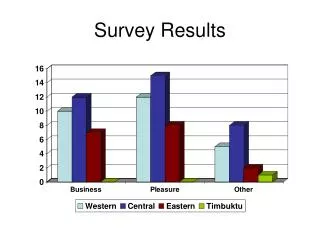
Two week response time • 195 people opened the survey • 162 people ranked top 4 responses • 97 people ranked all 12 • 14 people gave free text response
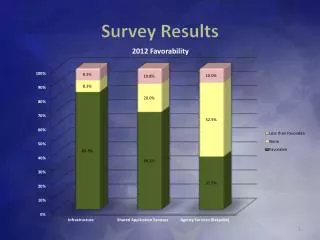
Rank-Weighting • A topic that was ranked 1st got 12 points • A topic that was ranked 12th got 1 point • The topics were then totalled
Free Text Responses “More fractured rotas lead to less training time and also less feeling of "belonging" and more of just "passing through" when rotating through different blocks. Whilst I welcome the improvement in hours that there has been over the last 9 years since I was a JHO working 90 hours a week we have reached a point where the quality of training is suffering.” “Academic training opportunities. More formalised clinical academic posts (not based around basic sciences but instead clinical research) in anaesthesia would be great.”
Free Text Responses “As an anaesthetic trainee that started in the 'old' system then completed anaesthetic and ITU training in Australia and is now back in the 'new' system, I have noticed a very large change in training offered, trainees attitudes and competency. Unfortunately not in a good way. The politicised training offered to comply with the EWTD and to push trainees through training to increase numbers of consultants on paper has had a very detrimental effect. Junior doctors (FY1/2 and a large proportion of ST1 and even 2's) are neither familiar nor capable at dealing with patient problems and are more and more learning to rush for help rather than deal with a situation. I definitely think that three years of core training should be mandatory as in paediatrics and the old SHO system and the RCOA should go back to not allowing anyone to sit the Primary prior to 12 months completed anaesthetic training. Consultant post are becoming more scarce in out deanery and increasing numbers of post CCT anaesthetists with less and less competency is not beneficial to the NHS or the individual - maybe an argument for the post CCT fellow as they have in NZ/Australia. With the consultant job plan having fewer and fewer SPA's and looking towards becoming resident on call these are looking less favourable anyway. Will the profession lose its best trainees to other specialties/regions or countries.”
Free Text Responses “Recruitment of overseas 'senior' anaesthetists to fulfil NHS work at significantly worse conditions than we expect. This is the single most significant problem for our generation of trainees, as it introduces unfair, non-market competition into our employment market. “ “Educational supervision and suitably rigorous RITA process. “ “The failure of our representative bodies (colleges/BMA) in particular to stand up for the profession and stop the debacle of MMC and the implementation of the EWTD. At least GAT tried to oppose MMC, the colleges were complicit and have never regained their credibility. The lack of Consultant posts and the number of trainees heading abroad to pursue their careers.”
Free Text Responses “Night working conditions and rota structure - many rotas now involve rapid and frequent switching between day and night shifts. It would be useful if GAT conducted a survey/research into optimising rota structures within the context of the EWTD to minimise the detrimental impact on sleep wake cycle. I believe that over the next few years there will be increasing evidence of the detrimental effects of night working and it would be good if we had some evidence to inform best practice for all medical specialties.” “Everyone does locums now, we are just as tired as pre-MTAS/EWTD days, but less experienced.” “Mental illness among anaesthetists”
Free Text Responses “The mindless application of box ticking exercises (DOPS etc.) replacing quality training. On rota gaps, if they exist it is up to Trusts to sort this out and fill them, not trainees - we are paid by deaneries to be trained (training budgets, there's another issue), while Trusts supply our banding to pay for out-of-hours service provision.” “Trainee assessments: There is little consistency in how these are conducted. The potential learning opportunity is often not fulfilled - just seen as a requirement for ARCP etc”
Free Text Responses “Senior trainees frequently being moved off useful training lists to cover last minute rota changes, because they are the only people available of suitable ability to cover these lists solo.” “Appropriate supervision of trainees. Flexible training. Inter-Deanery transfers. More flexibility within training programmes for secondments to allow acquisition of skills - eg ECHO training” “Covering intensive care for rota filling but not as ITU trainee”