Download
1 / 6
60 likes | 178 Views
DRAFT. BH Health Home October 18, 2012- Commission Meeting. PRELIMINARY WORKING DRAFT, SUBJECT TO CHANGE. 1. Health homes (& link to medical homes). 2. Episode-based care delivery. 3. 5. Reimbursement adjustments. Reimbursement for pharmacy (including polypharmacy). 4.

E N D
DRAFT BH Health Home October 18, 2012- Commission Meeting PRELIMINARY WORKING DRAFT, SUBJECT TO CHANGE
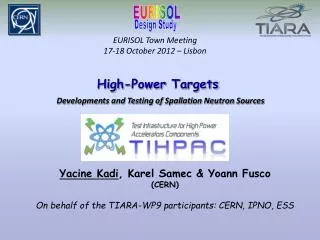
1 Health homes (& link to medical homes) 2 Episode-based care delivery 3 5 Reimbursement adjustments Reimbursement for pharmacy (including polypharmacy) 4 Reimbursement for new services 6 Policy changes/enabling initiatives Potential payment initiatives to address issues within the BH system PRELIMINARY Focus of today’s conversation
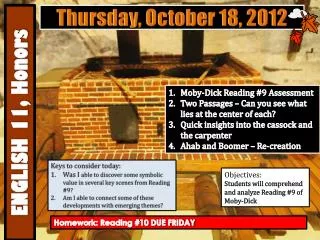
Key facts in behavioral health for the Medicaid population PRELIMINARY Early facts in Arkansas Definitions of key terms • “Core” behavioral health spend1: • Includes behavioral health services delivered to the client, (e.g., services for ADHD or depression) • Does not include direct dementia or DD costs, but does includes BH spend from these populations • Halo: • Includes non-behavioral health services (e.g., medical, support services) delivered to people who also use BH services Total Medicaid behavioral health beneficiaries ~110,000 recipients “Core” behavioral health spend ~$550 M “Halo” spend ~$380 M Pharmacy spend of behavioral health clients (BH and halo)2 ~$150 M NOTE: Does not include those funded solely from state general revenue. Analysis underway to incorporate broader behavioral health programs 1 Details of BH spend: ICD9 291 – 314 excluding autism (299) and dementia codes in 294, excludes pharmacy 2 Pharmacy includes some spend from some DD and dementia clients that has not yet been excluded SOURCE: 2011 Medical claims for behavioral health diagnosis codes. Does not include pharmacy, crossover or third party liability
Goals of the behavioral health health home PRELIMINARY • To deliver integrated care coordination in a manner that facilitates quality care and positive outcomes through: • Providing care coordination • Providing clients with integrated care coordination within and across BH, medical health, long-term supports, and other systems • Managing core care delivery • Ensuring effective treatment of behavioral health (BH) conditions, including pharmacy effects How can we design health home criteria and corresponding payment model to achieve these goals?
Guiding principles for health home development • Health homes must address comprehensive needs of individuals by utilizing a “whole person” and “person centered” approach while ensuring personal choice assurances through service planning and delivery • Health homes will provide services that address issues of access to care, accountability, and active participation on behalf of both providers and individuals/families receiving services, continuity of care across all medical, behavioral, and social supports, and comprehensive coordination/integration of all needed services • Health homes will provide services that seek to align a fragmented system of needs assessment, service planning, care coordination, transitional care, and direct care service delivery • Health homes must demonstrate the use of health information technology as a means to improve service delivery and health outcomes of the individuals served
Payment model • Which payment mechanisms can best incentivize system change (e.g., performance payments, care coordination fees)? • Considering how health home models will impact overall costs Performance measures • Developing ways to encourage positive performance in client care spanning core care delivery and care coordination • TBD Implementation & administration • Identifying external stakeholders and outline stakeholder (e.g., clients, providers, families) engagement activities • Identifying support and infrastructure required by behavioral health homes • Assessing system changes, state regulations, and internal DHS policies impacted by the implementation of a health homes Medicaid state plan option • Aligning health homes planning initiative with current health homes planning efforts in development by the DDS and the LTSS • Aligning health homes planning with PCMH planning efforts Key steps for BH health home design PRELIMINARY Elements in health home implementation Early list of activities from the BH health home workplan Target client population • Defining which behavioral health clients will benefit from health homes • Developing a methodology to identify the people who will likely have health homes • Determining applicability of assessment tools for health homes Health home activities • Defining health home activities • Integrating BH (includes mental health and substance abuse) and primary care, medical care, and long term services and supports • Addressing the needs of people with multiple diagnoses • Aligning the behavioral health homes with (i) delivery and payment for the delivery of core BH services (e.g., via episodes) and (ii) patient-centered medical homes Provider participation requirements • Outlining health home provider requirements • Developing provider certification criteria • Creating milestones for providers to transform practices and build health home capabilities Technology and infrastructure