Download
1 / 57
700 likes | 1.59k Views
Cough: Defense Mechanism and Symptom. Karen A. Fagan, MD Associate Professor of Medicine Chief of Pulmonary and Critical Care Medicine John and Alice Chair of Pulmonary Medicine University of South Alabama. Disclosure. No financial relationships relevant to this presentation or content

E N D
Cough:Defense Mechanism and Symptom Karen A. Fagan, MD Associate Professor of Medicine Chief of Pulmonary and Critical Care Medicine John and Alice Chair of Pulmonary Medicine University of South Alabama
Disclosure • No financial relationships relevant to this presentation or content • Any off label use of medications will be identified during the lecture
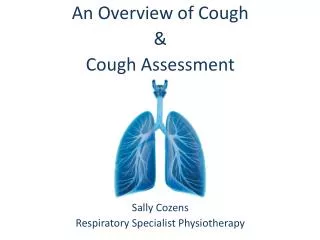
Objectives • Understand the function and physiological mechanisms of cough. • Classify cough according to its duration. • Know the most common causes of acute cough in adults. • Know the symptoms, signs, and empiric treatment for the 4 most common causes of chronic cough in adults.
Case Study- D.B. 47 y/o Caucasian woman, accountant, c/o cough for 3 years. 30 pack-year smoking history, quit in 2001. Traveled to China to adopt baby girl in 2002, caught “bad chest cold”. Recovered, but had “bronchitis” (phlegm, cough) ≥ 8 times/year thereafter. Episodes of “bronchitis” start suddenly, with a sore throat. Antibiotics and prednisone reduce symptoms, but incompletely. Coughs day and night. Told “you’re just getting a lot of colds from your daughter”. Frustrated. Worried about “weird infection.” Demoted at work because of days missed due to illness.
Case Study- D.B. • Review of Systems: + Mildly hoarse + Several sinus infections since 2002 - Heartburn, regurgitation - Cardiac disease - Neuromuscular disease • Physical Exam: Normal vital signs Looks depressed Otherwise, normal
Cough is #1 • The #1 chief complaint in primary care physicians’ offices is cough • Most-- but not all-- cough seen by PCP’s is acute cough related to viral upper and lower respiratory tract infections • Chronic cough is one of the most common reasons for consultation with a pulmonologist • Health care costs for cough exceed several billion dollars annually
Cough: What’s it good for? • Attract attention • Signal displeasure • Protect the airway from pathogens, particulates, food, other foreign bodies • Clear the airways of accumulated secretions, particles
Cough Reflex: Afferent Pathway • Vagus nerve is major afferent pathway • Stimuli arise from: • Ear • Pharynx • Larynx • Lungs • Tracheobronchial tree • Heart • Pericardium • Esophagus
Cough Reflex: Afferent Pathway Mechanical stimuli: • Rapidly adapting receptors (RARs) • Slowly adapting stretch receptors (SARs) • Chemical stimuli: • C-fibers
Efferent Pathway: 4 Phases 1. Inspiratory Phase 2. Compressive Phase 3. Expiratory Phase 4. Relaxation Phase
Impaired Cough: Who’s at risk? • Interruption of afferent and/or efferent pathways of cough reflex impairs cough • Altered sensorium- anesthesia, narcotics, sedatives, alcohol, coma, stroke, seizure, SLEEP • Laryngeal/ upper airway disorders • Tracheostomy tube • Restrictive and obstructive lung diseases • Neuromuscular diseases • Supine in hospital bed
Impaired Cough: Consequences • Aspiration of oropharyngeal or stomach contents (bacteria, food, other) • Acute airway obstruction • Pneumonia • Lung abscess • Respiratory failure/ ARDS • Bronchiectasis • Pulmonary fibrosis
Complications of Cough • Result primarily from marked increase in intrathoracic pressure (> 300 mmHg) during cough • Affect nearly every other organ system • See Table 1 (handout) for PARTIAL list • Disruption of surgical wounds • Negative impact on quality of life, particularly in chronic cough
Complications of Cough • Scares away big game! “The Silencer is a real hunt saver for: Spontaneous morning coughs Cold Flu and Allergy sufferers Asthma suffers Those on high blood pressure medications Excellent for Smoker's cough” www.biggameproshop.com
American College of Physicians 2006 Cough Guidelines • Evidence-based • Includes guidelines for pediatric cough • Should be used in conjunction with “clinical judgment” • Divides cough in adults by duration: acute, subacute, chronic
Acute Cough in Adults Cough lasting less than 3 weeks Key questions: 1. Is it life-threatening? 2. Are antibiotics needed?
Acute Cough History, Examination, Investigations Life-threatening Dx Non-life-threatening Dx Infectious Exacerbation of pre-existing condition Environmental or Occupational Pneumonia, severe exacerbation of asthma or COPD, PE, Heart Failure, other serious disease URTI LRTI Asthma Bronchiectasis UACS COPD Figure 1: The acute cough algorithm for the management of patients aged ≥ 15 years with cough lasting < 3 weeks. For diagnosis and treatment recommendations refer to the section indicated in the algorithm. PE = pulmonary embolism; Dx = diagnosis; Rx = treatment. For other abbreviations, see handout.
Acute Cough: Life-Threatening • Congestive heart failure • Pneumonia • Asthma Exac. • COPD Exac. • Pulmonary Embolism • Other
Acute Cough: Non-Life-Threatening • Upper respiratory tract infection (URTI or URI)-- “The Common Cold” • Caused by viruses, e.g. rhinoviruses • Nasal congestion, drainage • Post-nasal drainage irritates larynx • Inflammatory mediators increase sensitivity of sensory afferents • Antibiotics are NOT indicated • Decongestants, cough suppressants of questionable value
Acute Cough: Non-Life-Threatening • Lower respiratory tract infection-- “Acute Bronchitis” • Cough, with or without phlegm • Most bronchitis in otherwise healthy adults is caused by viruses (rhinovirus, adenovirus, RSV) • If it’s likely viral in origin, do not prescribe antibiotics • Bacterial causes to consider: • Mycoplasma pneumoniae, chlamydophila pneumoniae • Bordetella pertussis (whooping cough) • Make sure it’s not pneumonia
Acute Cough: Non-Life-Threatening • Exacerbation of pre-existing condition • COPD: always consider bacterial infection • Asthma: try to identify the underlying cause (exposure, viral URTI, viral LRTI, other) • Bronchiectasis: always consider bacterial infection (gram negative rods, staph. aureus, organisms resistant to antibiotics) • Upper airway cough syndrome (UACS) • Environmental or occupational exposure: allergens, irritants
Subacute Cough in Adults Key questions: 1. Is it post-infectious? 2. If post-infectious, are antibiotics needed? Cough lasting 3-8 weeks
Subacute Cough History and Physical Exam Post-infectious Non-postinfectious Workup same as chronic cough Pneumonia and other serious diseases New onset or exacerbation of pre-existing condition Pertussis UACS Asthma GERD Bronchitis Bronchitis NAEB AECB Figure 2: Subacute cough algorithm for the management of patients aged ≥ 15 years with cough lasting 3 to 8 weeks. For diagnosis and treatment recommendations refer to section indicated in algorithm. AECB = acute exacerbation of chronic bronchitis. For other abbreviations, please see syllabus.
Subacute Cough: Pneumonia
Chronic Cough in Adults • Cough lasting longer than 8 weeks • Top 4 in immunocompetent patient with normal CXR: • Upper airway cough syndrome • Asthma • Gastroesophageal reflux disease • Non-asthmatic eosinophilic bronchitis • Cough may have more than one cause-- a diagnostic challenge!
Upper Airway Cough Syndrome (UACS) • Also called “Post-nasal drip syndrome” (PNDS) • Mechanism: secretions from nose/sinuses stimulate upper airway cough receptors; inflammation increases receptor sensitivity • Classic symptoms: “tickle” in throat; throat clearing, hoarseness, nasal congestion • Cough may be the only symptom in ~ 20%
Upper Airway Cough Syndrome (UACS) • Signs(may be absent): inflamed nasal mucosa, secretions in posterior oropharynx • Consider underlying causes: allergies, chronic sinusitis, overuse of alpha-agonist nasal sprays • Diagnostic/Therapeutic trial: 1st generation anti-histamine/decongestant combination medication for 2 weeks
Asthma • Mechanism: inflammatory mediators, mucus, bronchoconstriction stimulate cough receptors • Classic symptoms: intermittent wheeze • Cough may be the only symptom in 7-57% patients (depends on study)-- “Cough-variant asthma” • Signs (often absent): expiratory wheezing on chest exam
Asthma • Diagnostic tests: • Spirometry, before and after bronchodilator: partially reversible airflow obstruction • Methacholine inhalation challenge: positive • Diagnostic/ • Therapeutic trial: inhaled corticosteroid + bronchodilator for • ≥ 8 weeks
A Vicious Cycle COUGH REFLUX INCREASED ABDOMINAL PRESSURE
Gastroesophageal Reflux Disease (GERD) • Classic symptoms: heartburn, sour taste in mouth • Cough may be only symptom in 75% patients with chronic cough • Diagnostic tests: • 24-hour esophageal pH probe (best) • Esophagram
Gastroesophageal Reflux Disease (GERD) • Diagnostic/Therapeutic trial: gastric acid suppression with proton pump inhibitor (e.g. omeprazole) for ≥ 2 months, combined with diet and lifestyle modification
Non-Asthmatic Eosinophilic Bronchitis (NAEB) • Eosinophilic airway inflammation WITHOUT variable airflow obstruction or airway hyperresponsiveness • Diagnostic tests: • Spirometry: normal • Methacholine challenge: • normal • Induced sputum: >3% eosinophils • Diagnostic/Therapeutic trial: inhaled corticosteroid for ≥ 4 weeks
Case Study: C.F A 67 y/o man, life-long non-smoker, complains of 12 weeks of non-productive cough. He’s had a couple of “colds” this winter. He has no current nasal or sinus symptoms, rarely has heartburn, and never wheezes. He’s on no meds. Vitals and physical exam are normal. Your next step would be: • Prescribe a 1st generation antihistamine/decongestant • Prescribe an inhaled corticosteroid for asthma • Order an induced sputum to look for eosinophils • Order a chest x-ray • All of the above
ACE-inhibitor therapy • Angiotensin converting enzyme (ACE) inhibitors (enalapril, captopril, lisinopril, ramipril, etc.) • Dry cough in 3-30% patients • Begins 1 week to 6 months after drug started • Usually resolves 1-7 days after stopping therapy, but can take 4 weeks
Bronchiectasis in patient with Common Variable Immunoglobulin Deficiency