Download
1 / 45
500 likes | 928 Views
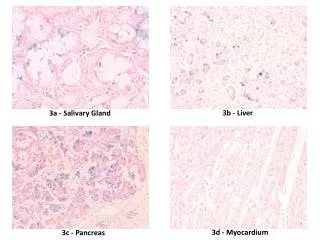
Salivary Gland Pathology. § Diagnosis of salivary gland disorders § Non neoplastic pathology • Metabolic conditions • Infectious conditions • Immunologic conditions § Neoplastic pathology § Postoperative complications. Diagnosis of Salivary Gland Disorders.

E N D
Salivary Gland Pathology • § Diagnosis of salivary gland disorders • § Non neoplastic pathology • • Metabolic conditions • • Infectious conditions • • Immunologic conditions • § Neoplastic pathology • § Postoperative complications
Diagnosis of Salivary GlandDisorders • Diagnosis of salivary gland disorders • is based on presenting signs and • symptoms, preexisting diseases, and • physical examination. • • plain-film radiography and sialography • to assist with diagnosis of nonneoplastic pathology • • CT and MRI to delineate the size and • extent of salivary neoplasms
Non-neoplastic Disorders • • Reactive conditions • • mucoceles and ranulas • • irradiation reactions • • sialolithiasis • • necrotizing sialometaplasia • • Infectious • • Nutrition disorders • • Medication reactions • • Immunologic disorders
Mucoceles • § Most common reactive condition of • the minor salivary glands • § Mucoceles form when trauma to • excretory ducts of the minor glands • allows the spillage of mucus into the • surrounding connective tissue • § formation of painless, smooth surfaced, • bluish lesions
§ The lower lip is the most frequent site followed by the buccal mucosa, the ventral surface of the tongue, the floor of the mouth, and the retromolar region § Treatment: • observation • surgical excision
Ranulas • § The result of blocked sublingual gland • ducts • § Ranulas are unilateral, soft-tissue lesions, • often with a bluish appearance. • § They vary in size and may cross the • midline of the mouth and cause deviation • of the tongue • § A mucosal extravasation that herniates • the mylohyoid muscle is called a • "plunging" ranula
Treatment of a Ranula Surgical excision of the involved gland and marsupialization • Marsupialization: suturing its walls to an adjacent structure, leaving the packed cavity to close by granulation
Irradiation Reaction • § A common side effect of tumoricidal • doses of ionizing radiation is xerostomia • § Frequent sips of water and frequent mouth • care are the most effective interventions • for xerostomia • § Saliva substitutes (eg, mixed solutions of • methylcellulose, glycerin, and saline) or • pilocarpine hydrochloride may help these • symptoms
Sialolithiasis • § Middle-aged patients most frequently • affected • § 85% of all salivary stones are located in • the submandibular gland • § Patients with sialolithiasis typically • complain of recurrent episodes of pain • and swelling when the gland is stimulated • to secrete, as when chewing food
Sialolithiasis • Treatment • • excision of salivary calculi from • Wharton's duct (ie, sialolithotomy) and • the administration of antibiotics for • underlying salivary gland infections • and/or excision of the entire submandibular • gland
Necrotizing Sialometaplasia • § Usually involves minor salivary glands • § Occurs secondary to vascular infarct due • to smoking, trauma, DM, vascular disease, • L/A • § Age range 23-66 yrs • § 1-4 cm ulceration • § resembles mucoepidermoid carcinoma • and SCCA clinically and histologically • § Usually heal in 6-10 weeks
Nutrition Disorders • § Nutrition disorders such as pellagra (ie, • niacin deficiency), kwashiorkor (ie, protein • deficiency), beriberi (ie, thiamine • deficiency), and vitamin A deficiency are • associated with parotid gland enlargement • § Malabsorption syndromes also can cause • malnutrition and result in salivary gland • dysfunction
Medication Reactions • Many medications (eg, amitriptyline, • imipramine, nortriptyline, atropine, • phenothiazine derivatives, • antihistamines) decrease salivary • flow and cause parotid enlargement
Metabolic Conditions • § Patients with alcoholic cirrhosis often • experience asymptomatic enlargements of • their parotid glands, which are attributed • to chronic protein deficiency • § Diabetes mellitus and hyperlipidemia • cause fatty infiltrations that replace the • functional parenchyma of the salivary • glands and decrease the flow of saliva
Infectious Conditions • § Mumps • § Cytomegalovirus (CMV), which is a • DNA virus of the herpes family that is transmitted by human contact
Bacterial infectionsacute and recurrent chronic sialadenitis • § Etiology: Staphylococcus aureus, • Staphylococcus pyogenes, Streptococcus • pneumoniae, and Escherichia coli • § Predisposing factor: reduction in salivary • flow (ie, secondary to dehydration, • debilitation, medication side effects) • § Treatment is directed at elimination of the • causative agent, rehydration of the • patient, and surgical drainage of • purulence when indicated
Immunologic conditions • § HIV may manifest with parotid gland • enlargement and parotid • lymphadenopathy often are observed in • these immunocompromised patients.
Sjogren's syndrome • § Autoimmune disorder characterized • by a chronic inflammatory reaction of • exocrine glands +/or systemic • connective tissues • § Sjogren's syndrome includes any of • the three findings: • • keratoconjunctivitis sicca (ie, dry eyes) • • ` salivary gland enlargement, and xerostomia • • vasculitis • • purpura • • hepatosplenomegally • • obstructive pulmonary disease • • anemia • • rheumatoid arthritis
Neoplasms • § Salivary neoplasms generally present as • painless, slow-growing masses • § Neoplasms of the major salivary glands • usually are benign • § Neoplasms of the minor salivary glands • usually are malignant • § Rapidly expanding salivary neoplasms • that are associated with pain and neural • dysfunction are more likely to be • malignant
85% of salivary neoplasms arise in the parotid § 10% in the submandibular gland § 5% in the minor salivary glands § Salivary neoplasms rarely occur in the sublingual glands
Benign salivary neoplasms • Histologically, benign neoplasms are • classified as: • • pleomorphic adenomas / benign mixed tumors • • papillary cystadenolymphomas /Warthin's tumors • • oncocytomas • • monomorphic adenomas • • benign lymphoepithelial lesions
Benign salivary neoplasms • § The most common benign neoplasm • is pleomorphic adenoma • § parotid gland 92.5% • § submandibular gland 6.5% • § The treatment of choice for benign • neoplasms is surgical excision
Malignant salivary neoplasms • Malignant salivary neoplasms are classified • as: • • malignant mixed tumors • • mucoepidermoid carcinoma • • adenocarcinoma • • acinic cell carcinoma • • squamous cell carcinoma • • adenoid cystic carcinoma • • metastatic melanoma
Malignant salivary neoplasms • § Surgery is the treatment of choice for • resectable malignant salivary neoplasms • § Surgeons also may perform neck • dissections if lymph node involvement is • present or suspected • § Postoperative radiation therapy may be • used as an adjunctive treatment to • eradicate microscopic or residual disease
Complications • § Xerostomia • § Hemorrhage • § Temporary facial nerve paralysis 15% • § Long-term facial nerve paralysis • § Frey's syndrome
Salivary Gland Disorders • § Clinicians are frequently confronted • with the necessity of assessing and • managing salivary gland disorders • § This basic knowledge of salivary • gland anatomy, physiology, • pathophysiology is necessary to • treat your patients properly