Download
1 / 12
120 likes | 269 Views
The Surgical Completeness of Robotic thyroidectomy : A prospective Comparative Study of Robotic versus conventional open thyroidectomy in papillary thyroid carcinoma patients.

E N D
The Surgical Completeness of Robotic thyroidectomy : A prospective Comparative Study of Robotic versus conventional open thyroidectomyin papillary thyroid carcinoma patients Sohee Lee M.D., Seulkee Park M.D., Cho Rok Lee M.D., Haiyoung Son M.D., Jungwoo Kim M.D., Sang-Wook Kang M.D., JongJuJeong M.D., Kee-Hyun Nam M.D., WoongYoun Chung M.D. and Cheong Soo Park M.D. Department of Surgery Yonsei University Health System, Seoul, Korea
Introduction • Conventional open thyroidectomy with direct approach through the neck • Most Effective and safe method • Noticeable scar in highly visible area
Introduction • Robotic thyroidectomy via transaxillary approach • Excellent cosmesis • Short term outcome : comparable with conventional open thyroidectomy in low risk papillary thyroid cancer patients
Introduction • The oncologic safety with surgical radicality of robotic thyroidectomy should be prior to cosmesis in managing thyroid cancer • Robotic thyroidectomy via trans axillary approach has been criticized about complete excision of contralateral lobe • The aim of this study : to show the surgical completeness of robotic thyroidectomy by comparing with conventional open thyroidectomy in papillary thyroid carcinoma
Patients and Methods • 110 patients with papillary thyroid carcinoma were enrolled from April, 2009 through February 2011 • All underwent total thyroidectomty and 30 mci RAI ablation therapy • 55 underwent conventional open thyroidectomy 55 underwent robotic thyroidectomy • Definite extrathyroidal tumor invasion, lateral neck node metastases, perinodal infiltration at a metastatic lymph node, or distant metastasis were excluded
Patients and Methods • Tumor located in the thyroid dorsal area (particularly at the tracheoesopheal groove) with posterior capsular invasion or extension to an adjacent structure were also excluded in robotic thyroidectomy • Extent of surgery : According to the ATA guidelines Prophylactic ipsilateral CCND : performed for all the patients • 12 patients were excluded ( ex. pregnancy, pt’s refusal) : three open thyroidectomy nine robotic thyroidectomy • Analysis of surgical completeness : • Radioiodine uptake • Postoperative serum Tg level
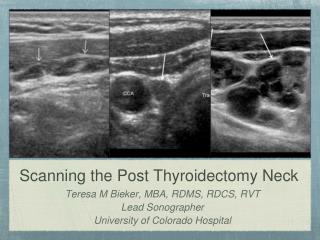
Patients and Methods • Radioactive iodine uptake calculate RAI uptake (%) in thyroid bed area (thyroid/whole body, thyroid/brain) • 30mci RAI ablation therapy at postoperative 2~3 months • Diagnostic scan at 1 year after 1st RAI ablation • Before 131-I Tx, at least 3-4 weeks Levothyroxine withdrawal with low iodine diet or rhTSH administration • pre RAI TSH level > 30 μIU/mL
Patients and Methods • Serum Tg level • TSH stimulated Tg at 1st RAI ablation and diagnostic scan • TSH suppressed Tg : 6 month after RAI therapy • The patient’s clinicopathologic characteristics, surgical outcomes, RAI uptake, serum Tg level were compared between the two groups.
Results † Diagnostic scan was performed at 12months later after 1st RAI ablation
Conclusion • Robotic thyroidectomy showed significant high uptake at RAI ablation therapy compared with conventional open thyroidectomy. • However, stimulated Tg level at RAI therapy showed no significant difference between two groups. • Remnant thyroid tissue after robotic thyroidectomy can successfully managed by 30mci RAI ablations. (RAI uptake, stimulated Tg at diagnostic scan show no differences between two groups.) • Robotic thyroidectomy is safe and feasible in managing low risk papillary thyroid carcinoma patients
Thank you for your attention