Download
1 / 58
630 likes | 947 Views
Scanning the Post Thyroidectomy Neck. Teresa M Bieker, MBA, RDMS, RDCS, RVT Lead Sonographer University of Colorado Hospital. Objectives:. Appearance of Normal Cervical Lymph Nodes Appearance of Abnormal Cervical Lymph Nodes Identifying Zones/Levels of the Neck

E N D
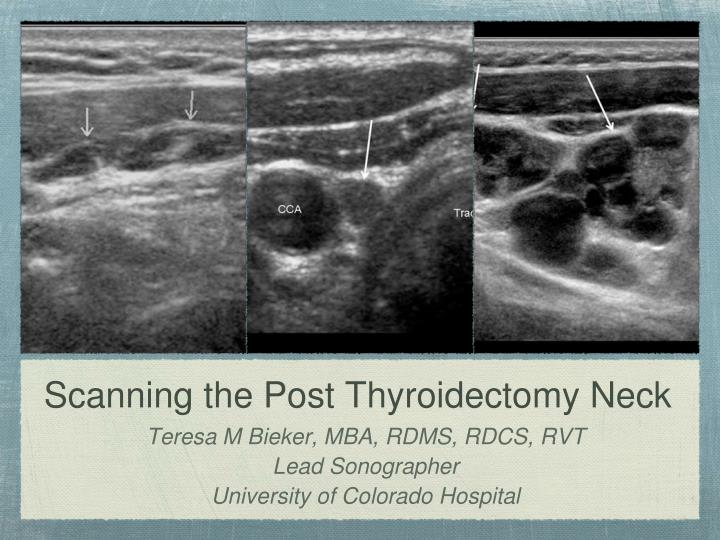
Scanning the Post Thyroidectomy Neck • Teresa M Bieker, MBA, RDMS, RDCS, RVT • Lead Sonographer • University of Colorado Hospital
Objectives: • Appearance of Normal Cervical Lymph Nodes • Appearance of Abnormal Cervical Lymph Nodes • Identifying Zones/Levels of the Neck • Scanning Technique and Protocol
Background: • Thyroid cancer is the most common endocrine cancer • In 2011, there where 48,020 new cases (26,550 women, 11,470 men) and 1,740 deaths • For 2013, American Cancer Society estimates 60,220 new cases (46,970 women, 13,250 men) and 1,850 deaths • Two thirds of patients are between 20-55 with a mean age of 45 • Causes include: • occupational risks • diet • lifestyle • parity • family history
Types of Thyroid Cancer: • Well Differentiated Thyroid Cancer: • Papillary • Follicular • Arise from thyroid follicular cells • Account for 80-90% of all thyroid cancers • Poorly Differentiated Thyroid Cancer: • Medullary (5-10%) • Anaplastic (1-2%)
Outcomes: • Thyroid cancer is treatable; however, outcome is dependent on stage (I-IV) • Five year survival rates: • Papillary: 51% to >99% • Follicular: 50% to >99% • Medullary: 28% to near 100% • Anaplastic: 7%
Factors Affecting Treatment/Outcomes: • Age • Distant metastasis • Local invasiveness • Cervical lymph node metastasis • Tumor size • Multifocality • Tumor subtype
TNM Classification: • T = Tumor • N = Node • M = Distal Metastasis
TNM Classification TX: Primary tumor cannot be assessed T0: No evidence of primary tumor. T1: Tumor ≤2 cm in greatest dimension limited to the thyroid. T1a: Tumor ≤1 cm, limited to the thyroid. T1b: Tumor >1 cm but ≤2 cm in greatest dimension, limited to the thyroid. T2: Tumor >2 cm but ≤4 cm in greatest dimension, limited to the thyroid. T3: Tumor >4 cm in greatest dimension limited to the thyroid or any tumor with minimal extrathyroid extension (e.g., extension to sternothyroid muscle or perithyroid soft tissues). T4a: Moderately advanced disease. Tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve. T4b: Very advanced disease. Tumor invades prevertebral fascia or encases carotid artery or mediastinal vessels
TNM Classification: • NX: Regional lymph nodes cannot be assessed. • N0: No regional lymph node metastasis. • N1: Regional lymph node metastasis. • N1a: Metastases to Level VI (pretracheal, paratracheal, and prelaryngeal/Delphian lymph nodes). • N1b: Metastases to unilateral, bilateral, or contralateral cervical (Levels I, II, III, IV, or V) or retropharyngeal or superior mediastinal lymph nodes (Level VII)
TNM Classification: • M0: No Distant metastasis • M1: Distant metastasis
Recurrence Rates: • For well differentiated thyroid cancer, there is a 9-30% recurrence rate within the first decade after diagnosis • Most recurrences occur within the thyroid bed or cervical lymph nodes • 60-75% occur in Z3 or Z4 • 20% occur in Z6 • Tend to affect the ipsilateral neck
Surgery: • Total or near total thyroidectomy is the standard treatment for thyroid cancer. Z6 lymph nodes can also be removed at this time • If the lateral/cervical lymph nodes are involved, a neck dissection is also performed • Ultrasound and FNA are essential for surgical management
Post Operative Evaluation: • Physical palpation exam by endocrinologist/surgeon • Depending on extent of disease: • Iodine 131 whole body scan • Radioactive iodine ablation therapy • Chest x-ray • CT/MRI/PET • Neck ultrasound/Labwork (6-12 months)
Labwork: • Typically drawn every 6-12 months • Thyroglobulin (Tg) • Specific protein secreted from thyroid tissue • Tg levels should be undetectable in disease free patients • If Tg increases, it is likely caused by recurrent tumor • Tg Antibodies • Present in 20-25% of thyroid cancer patients • If antibodies are positive, Tg levels are falsely decreased • Tg antibodies typically decrease over several years • When disease in present, antibodies can increase • Thyroid Stimulating Hormone (TSH) - suppressed by medication
Lymph Nodes: • There are approximately 300 lymph nodes in the neck • Normal nodes have a cortex and medulla covered by a fibrous capsule • Cortex: contains lymphocytes packed together forming spherical lymphoid follicles • Medulla: contains trabeculae and medullary cords and sinuses. Multiple medullary sinuses form the echogenic hilum • A main artery and vein enter/exit the node at the hilum
Cervical Lymph Nodes: • jnccn.org
Lymph Node Anatomy: training.seer.cancer.gov
Lymph Nodes: • Common Locations • Normal Appearance • Abnormal Appearance
Common Lymph Node Locations: • Arranged in chains • Commonly visualized along: • Jugular chain • Submandibular gland • Supraclavicular region • Thyroid bed
Why Ultrasound? • ATA recommends U/S pre and post thyroidectomy • More sensitive in detecting lymph nodes and determining benign vs malignant • More cost effective • Quicker, non-invasive • No radiation • Can detect disease as small as 2-3mm (often before palpated or detected by Tg) • FNA • Very operator dependent
Post Thyroidectomy Scanning: • 12-15 MHz, 8MHz curved • Patient Position • Supine with neck extended • Elevating the head 20o in obese patients may help • Neck rotation • Image optimization
Post Thyroidectomy Scanning: • Indications: • Routine screening • Elevated TG • Follow-up • Correlation with NM, CT, PET • Zones 1-7 are evaluated and imaged • Residual thyroid tissue • Recurrent thyroid tumor • Abnormal lymph nodes
Cervical Lymph Nodes: • It is not unusual to see multiple normal nodes in the neck • The number of normal nodes visualized increases with age • Characterized by: • Location • Shape • Size • Echogenicity • Vascular pattern • Presence of echogenic hilum
Normal Lymph Nodes: • Hypoechoic cortex • Echogenic hilum • Strong predictor of a normal node • Maybe difficult to visualize in small nodes • One feeder vessel (hilar flow) • Cylindrical or cigar shape
Abnormal Lymph Nodes: • Lose elliptical shape and become more rounded • Malignant cells invade the node, disrupting the hilum • 96% of malignant nodes lack a fatty hilum • Become hyperechoic with papillary invasion but hypoechoic with medullary and lymphoma. • Increase in echogenicity due to the presence of Tg within the lymph node • Microcalcifications • Mixed or peripherial flow • Cystic in advanced disease
Lymph Node Doppler: • Hilar: flow branches radially from the hilum • Peripheral: flow is present along the periphery of the node but does not arise from the hilar vessels • Mixed: hilar and peripheral flow • Absence of flow despite optimal Doppler settings • Literature is inconsistent on benefit of color and pulsed Doppler
Zone 6 Abnormalities: • Following thyroidectomy, the paratracheal region should be homogeneous • Z6 masses can include: • Postoperative scarring • Muscle • Necrosing fat • Suture granulomas • Parathyroid gland • Lymph node • Remnant tissue • Metastasis
Zone 1: • Medial or anterior to the SMG • Midline/superior to hyoid bone • Nodal group: submental/submandibular • Unusual to have papillary involvement in Zone 1 • Often see reactive nodes
Zone 6: • Anterior/medial to the CCA • From the hyoid inferiorly to the manubrium • Nodal group: anterior cervical nodes, pre and para tracheal • 20% of recurrences are in Zone 6
Zone 2: • Lateral/posterior to the SMG • Superior to the hyoid bone (CCA bifurcation) • Nodal group: upper IJ chain, parotid nodes • Reactive nodes can be seen in Zone 2 • Uncommon for PTC, but can occur
Zone 3: • From the level of the hyoid (CCA bifurcation) to the cricoid cartilage (level of expected thyroid bed) • Lateral to CCA • Nodal group: middle IJ chain • 60-75% of recurrences are in Zone 3 or 4
Zone 4: • From the cricoid arch to the level of the clavicle (thyroid bed level) • Lateral to the CCA • Nodal group: lower IJ chain • 60-75% of recurrences are in Zone 3 or 4
Zone 7/Notch: • Anterior/ medial to CCA • At or inferior to the sternal notch • Nodal group: anterior, upper mediastinal nodes • Zone 7 vs Notch: • Zone 7 is inferior to the subclavian • This changes surgical management. “Notch” nodes can be removed during standard thyroidectomy. Zone 7 nodes requires a more extensive surgery
Supraclavicular: • Lateral to the CCA • At or inferior to the clavicle • Nodal group: supraclavicular nodes