Download
1 / 52
520 likes | 548 Views
Explore the detailed process of heart development from the formation of the heart tube to looping and differentiation stages. Understand the critical stages and structures involved in early heart development, including the contribution of different mesodermal layers and the formation of essential cardiac structures. Learn about the intricate process of folding and fusion that shapes the heart structure.

E N D
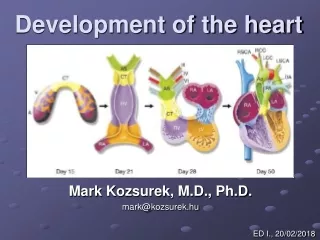
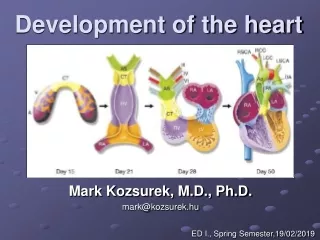
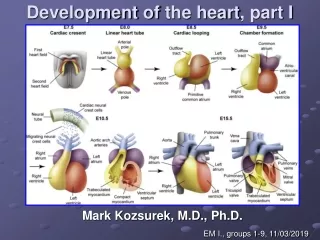
Development of theheart, part I Mark Kozsurek, M.D., Ph.D. EM I., groups 1-9, 11/03/2019
Development of theheartincludes: • formation of thehearttube, • looping and furtherdifferentiation of thehearttube, • partitioning of theheart – completeisolationoftheleft and right halves, • formation of thevalves.
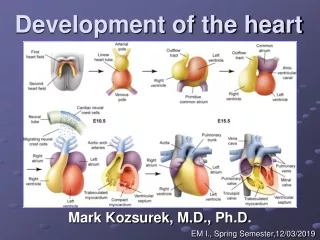
I. Earlydevelopment of theheart: appearance of the heart tube Heart primordium appears on the 18th-19th days (the end of the third week). At this stage the embryo is a flat, trilaminar disc and the differentiation of the three germ layers has just begun. Heart develops from the cardiogenic area, a part of the intraembryonic mesoderm anterior to the oropharyngeal membrane.
Note that heart starts to develop anterior to the brain! brain spinal cord
oropharyngeal membrane cloacal membrane amniotic cavity yolk sac extraembryonic celom chorion septum transversum connecting stalk notochord cardiogenic area
Within the cardiogenic area the first and second heart field appears (both of them have intraembryonic mesodermal origin). First heart field gives atria and the left ventricle,while from the second one the right ventricle and the conotruncal region (CT: bulbus cordis and truncus arteriosus) develops. Immigrating neural crest cells also contribute to the formation of the aortic sac (AS).
lateral plate mesoderm somatic layer splanchnic layer intraembryonic celom amniotic cavity yolk sac cardiogenic area
angioblastic cords somatic layer somatic layer splanchnic layer splanchnic layer splanchnic layer A group of cells leaves the splanchnic mesoderm, moves medially and forms the angioblastic cords.
myoepicardial mantle somatic layer splanchnic layer endocardial tubes On the dorsal side of the endocardial tube, the splanchnic mesoderm thickens and forms the myoepicardial mantles.
Further development of the heart is mainly determined by the folding of the embryo (4th week). The folding includes: 1) folding around transverse axes – this will explain, how the heart primordium moves from „above the head” into the chest occupying its final position. 2) folding around the longitudinal axis – this will mainly explain the fusion of the structures originally developing on the two sides of the embryo.
foregut dorsal mesocardium intraembryonic celom pericardial cavity Folding around the longitudinal axis
Folding of the embryo results in the fusion of the two endocardial tubes in the midline. Somewhat later the myoepicardial mantles also unite and surround the endocardial tube. The intraembryonic celoms fuse ventrally, and finally, the dorsal mesocardium disappears.
The heart tube, branching both rostrally and caudally, is surrounded by the pericardial cavity.
Summary • Cells emigrating from the splanchnic mesoderm form the endocardial tubes, this gives later the ENDOCARDIUM. • Thickening of the splanchnic mesoderm gives the myoepicardial mantles from which the MYOCARDIUM, and the VISCERAL LAYER OF THE PERICARDIUM (EPICARDIUM) develop. • Intraembryonic celom, originally bounded by the lateral plates, transforms into the PERICARDIAL CAVITY. • Somatic layer of the mesoderm differenciates into the PARIETAL LAYER OF THE PERICARDIUM.
As the two ends of the heart tube are fixed, its intense longitudinal growth necessarily results in the formation of several loops and curvatures. Furthermore some parts of the tube remain narrower, while others dilate. The venous end moves backward and ascends and gets behind the slightly descending arterious end. TA TA TA BC CA CV CV CA LV RV SV SV SV (anterior view; SV: sinus venosus, CA: common atrium, CV: common ventricle, BC: bulbus cordis, TA: truncus arteriosus)
cardiogenic plate endocardial tubes and their fusion 6 5 4 3 1- 6 6 • sinus venosus • commonatrium • atrioventricularcanal • commonventricle • bulbuscordis • truncusarteriosus 4 5 4 3 5 Common ventricle gives the later LV and the inflow part of the RV, while the bulbus cordis differentiates into the outflow part of the RV! RV 3 2 LV 2 1 1
sup. post. ant. inf. truncus arteriosus sinus venosus TRANSVERSE SINUS common atrium bulbus cordis atrioventricular canal common ventricle OBLIQUE SINUS
left sinus horn sinus venosus right sinus horn sinu-atrial opening truncus arteriosus sinusvenosus common atrium common atrium bulbus cordis atrioventricular canal lateral view atrioventricular canal Note the right and left sinus horns draining into the sinus venosus and the right and left veinous valves (green) at the sinu-atrial opening! common ventricle common ventricle frontal view
sinus venosus left sinus horn → coronary sinus truncus arteriosus right sinus horn sinusvenosus sinu-atrial opening bulbus cordis common atrium common atrium common ventricle atrioventricular canal atrioventricular canal The sinu-atrial opening moves to the right, the left sinus horn (or duct of Cuviér) involutes and persists as the coronary sinus. common ventricle
SVC left sinus horn → coronary sinus truncus arteriosus sinus venarum sinusvenosus sinu-atrial opening bulbus cordis common atrium IVC common atrium common ventricle atrioventricular canal atrioventricular canal Note the three veins opening into the sinus venarum (derivative of the sinus venosus): the superior and inferior vena cava and the coronary sinus! common ventricle
SVC pulmonaryveins coronary sinus truncus arteriosus sinus venarum sinusvenosus sinu-atrial opening bulbus cordis common atrium IVC common atrium common ventricle atrioventricular canal atrioventricular canal Pulmonary veins arise from (or enter) the left portion of the common atrium. common ventricle
SVC pulmonaryveins coronary sinus truncus arteriosus sinus venarum sinusvenosus sinu-atrial opening bulbus cordis common atrium IVC common atrium common ventricle atrioventricular canal SMOOTH ROUGH atrioventricular canal Sinus venarum and pulmonary vein segments getting incorporated into the atrial wall will give the smooth-walled parts of the atria (blue), while the original regions of the common atrium will persist as the rough parts of the atria. common ventricle
Septation of thecommonatrioventricular (AV) orifice. • Formation of theinteratrialseptum. • Formation of themuscularinterventricularseptum. • Appearance of themembranousinterventricularseptum and thespiralaorticopulmonaryseptum. 2nd lecture today
septum primum septum primum
septum primum septum primum
septum primum septum primum foramen primum foramen primum
septum primum septum primum foramen primum foramen primum
septum primum septum primum foramen secundum foramen secundum foramen primum foramen primum
septum primum septum primum foramen secundum foramen secundum foramen primum foramen primum
septum primum septum primum foramen secundum foramen secundum
septum secundum septum secundum foramen secundum foramen ovale septum primum foramen ovale septum primum
septum secundum septum secundum foramen secundum foramen ovale septum primum foramen ovale septum primum
septum secundum septum secundum foramen secundum septum primum foramen ovale foramen ovale septum primum
limbus: septum secundum base of fossa ovalis: septum primum
Summary • The septation of thecommonatriumstartswiththeappearance of thecrescent-shapedseptumprimum. The opening of thisseptum, theforamenprimum, becomesprogressivelysmaller. • Beforetheforamenprimumcompletlycloses, postero-superiorlyseveralsmallopeningsappearontheseptumprimum. Theseperforationscoalescelater and formtheforamensecundum. • Ontherightside of theseptumprimum a newseptum, theseptumsecundum, startstogrow. The orifice of theseptumsecundum is theforamenovale. • Finallytwocrescent-like, incomplete, partially overlapping septaexistwithoneholeoneach. Septumsecundum is more rigid and theseptumprimumonitsleftsideactsas a valve letting theblood flow exclusivelyfromtherighttotheleft. Itsimportancewillbecomeobviouswhenthefetalcirculation is discussed.
The fate of SA valves (right and leftvenousvalves)
Right and leftvenousvalves: twosemilunarstructuresatthesinu-atrialjunction. Postero-superiorlytheyunite and formtheseptumspurium. The leftonelatercompletlydisappearsbyfusingwiththeinteratrialseptum. The rightonedividesintotwo: theupper part persistsas a part of thecristaterminalis, whilethelowergivesthemass of theThebesian and theEustachianvalves.
As they are all derived from the same structure, valves of IVC and coronary sinus as well as the crista terminalis can be marked with one uninterrupted line!