Download
1 / 95
1.03k likes | 1.45k Views
Urogenital trauma Dr.N.Sridharan , Urologist . Sabah Al Ahmad Urology Center. Urogenital trauma. External trauma Iatrogenic injury. Urogenital trauma. Kidney Ureter Bladder Urethra External genitalia. External trauma. Mechanism of Injury Clinical symptoms and signs

E N D
Urogenital traumaDr.N.Sridharan, Urologist Sabah Al Ahmad Urology Center
Urogenital trauma • External trauma • Iatrogenic injury
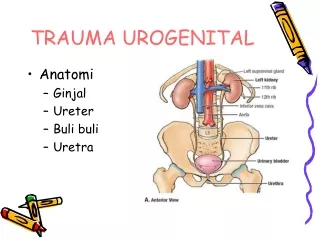
Urogenital trauma • Kidney • Ureter • Bladder • Urethra • External genitalia
External trauma • Mechanism of Injury • Clinical symptoms and signs • Investigations / Imaging • Grading system • Management
Great Foley debate • When to insert a Foley catheter • When NOT to insert a Foley catheter
External trauma • 4 – 10 % of accident patients coming to Emergency room(ER) will have Urogenital trauma. • More than 80 % - managed conservatively.
External trauma • Kidney – 67% • Ureter – 1% • Bladder –22% • Urethra – 3% • External genitalia – 7%
Kidney Injury • Blunt trauma (90 – 95 %) • Road traffic accidents • Fall from height • Assault • Penetrating injury – upper abdomen or lower chest • Stab wounds • Gun shot wounds
Mechanism of Injury • High velocity impact ( Acceleration injury) • Contusion • Hematoma • Laceration • Deceleration injury • Renal artery thrombosis • Renal vein disruption • Renal pedicle avulsion
When do you suspect Renal Injury • Trauma to back / flank / lower thorax / upper abdomen • Flank pain / Hematuria • Ecchymosis over the flanks • Suddendeceleration / Fallfromheight. • Lumbar transverse process # / lowrib #
Lumbar Transverse Process Fractures • Abdominal organ injuries - 47% • Kidney: 1/3 • Liver: 1/3 • Spleen: 1/4 Lumbar transverse process fractures: a sentinel marker of abdominal organ injuries. Injury. 31:773; 2000. Miller et al.
Clinical symptoms and signs • First sample of urine post trauma is important • Frank Haematuria - very significant • Microscopic haematuria – more than 5 RBCs/hpf
ABCDE A - airway with cervical spine protection B - breathing C - circulation and control of external bleeding D - disability or neurologic status E - exposure (undress) and temperature control ( American College of Surgeons Committee on Trauma, 1997 ).
Imaging required • Gross haematuria- Blunt trauma • Microscopic Haematuria • Blunt trauma + Systolic BP below 90 mm Hg • Penetrating injury with any haematuria • Paediatric patients with any haematuria • Absence of hematuria but high clinical index of suspicion of renal injury • Rapid deceleration injury • Lower rib # • Transverse process # • Loss of psoas shadow
Imaging of choice • CT Abdomen and pelvis with Contrast • CT films in first 2-3 minutes after contrast injection • Delayed CT at 10 minutes to study for collecting system , pelvis and ureter • CT cystogram if bladder injury suspected
American Association for the Surgery of Trauma Organ Injury Severity Scale for the Kidney[*] * Data drawn from Moore EE, Shackford SR, Pachter HL, et al: Organ injury scaling: Spleen, liver, and kidney. J Trauma 1989;29:1664-1666
Organ Injury Severity Scale • Validated: Journal of Trauma, 2001 • Predicts the need for surgery • Need for surgery ; nephrectomy rates: • Grade I: 0 ; 0% • Grade II: 15 ; 0% • Grade III: 76 ; 3% • Grade IV: 78 ; 9% • Grade V: 93 ; 86% Santucci et al. Validation of the American Association for the Surgery of Trauma OrganInjurySeverityScale for the Kidney. J Trauma; 50:195-200; 2001.
Renal Trauma CT Findings – Major Trauma • Urinary extravasationmedial to kidney • Suggests UPJ avulsion or renal pelvic injury • Hematoma medial to kidney, displacing kidney laterally • Suggests pedicle injury • Lack of contrast enhancement of kidney • Suggests arterial injury
In unstable patients During laparotomy - Significant retroperitoneal haematoma • Patient unstable even after intraperitoneal bleed managed. • Pulsatile /Expanding retroperitoneal haematoma • “Single-shot” intraoperative IVP (2cc/kg IV contrast) • Single film taken 10 minutes after IV injection
Intra operative one shot IVP • Confirms existence of other kidney • Highly specific for urinary extravasation • Allows safe avoidance of renal exploration in 32% (Morey et al 1999)
Management • Conservative in more than 80 – 90 % of cases. • Grade I – III • Grade IV : +/- • Strict bed rest • Monitor vital signs • Serial haematocrit measurement • Follow up ultrasound / CT scan • Ambulation allowed only after gross haematuria settles
Grade III Renal Injury Plain CT Contrast CT Reconstruction
Renal Injury – Conservative management Gr III Renal Injury 4 weeks later
Indications for surgery • Absolute indications • evidence of persistent renal bleeding ( > 2 units / day) • expanding perirenal hematoma • pulsatileperirenal hematoma • Relative indications • urinary extravasation • nonviable tissue (more than 20 %) • delayed diagnosis of arterial injury • segmental arterial injury • incomplete staging • Most penetrating / Gun shot injury ( McAninch et al, 1991 ).
Renal exploration • ALWAYS midline abdominal incision • Inspection of intra abdominal organs and bowel by the surgeons – FIRST STEP
Early renal vessel Isolation • Expose the aorta in the mid retroperitoneum • Secure the renal vessel with a tape • Open Gerota’s fascia lateral to colon afterwards • Renal salvage rate - 88 %. McAninch and associates (1991)
Principles of renal reconstruction after trauma • Complete renal exposure • Débridement of nonviable tissue • Hemostasis by individual suture ligation of bleeding vessels • Watertight closure of the collecting system • Coverage or approximation of the parenchymal defect
Renal Trauma Technique of Renal Reconstruction
URETER – Mechanism of injury • External trauma – Rare (<20 %) • Iatrogenic (common – 80%) • Almost always associated intra abdominal organ injuries • Stab wounds/Gun shot wounds • Blunt – very rare - rapid deceleration injury - esp. in falls - in children (UPJ avulsion)
Location Varies depending on mode of injury • External trauma – Upper -39% Mid – 31% Lower-30% • Blunt – UPJ • Iatrogenic – Distal ureter
Diagnosis - clinical IMMEDIATE • Hematuria – unreliable sign Present in only 50% of ureteral trauma • Blunt – suspect in hyperextension or decelaration injury, esp in children,fall from height
Delayed presentation • Prolonged ileus • Fever/Sepsis • Persistant flank/abdo pain/mass • Urine leak,prolonged drain output • Anuria,raised renal parameters
High index of suspicion • Low threshold for imaging • Delayed diagnosis = Increased complications
Diagnosis in Penetrating Inj- Imaging • IVP 1 shot IVP unreliable (accuracy 38%) Complete IVP (accuracy 61%) UCNA Feb 2006 • Retrograde Pyelogram (RGP) Sensitive and specific Limited use in acute setting • CT – Insufficient data (BJU 2004)
Grading – AAST Grade Type of Injury Description of Injury I Hematoma Contusion or hematoma without devascularisation II Laceration <50% transection III Laceration >50% transection IV Laceration Complete transection with less than 2cm devascularisation V Laceration Avulsion with more than 2cm devascularisation (Advance one Grade for bilateral – uptoGr III)
Management of Penetrating inj • Minimal Contusion – Ureteric stent • Severe Contusion – Segmental excision & Uretero-ureterostomy
Management of Penetrating inj • Delayed • PCN -> Antegrade stent • Retrograde stent often unsuccessful • Urinomas • PCN
Blunt trauma • CT with delayed films diagnostic • Medial perirenalextravasation • Unopacified ureter • Intact renal parenchyma • Lack of perirenal (lateral) hematoma
Management of blunt trauma • UPJ common, followed by upper ureter • Partial – Primary repair + ureteric stent • Complete – Ureteropyelostomy/UU
Management in unstable patient • Delay ureteric repair until stable • Ureteric ligation and PCN • Ureterostomy
Ureteral Injuries – Surgical options • Upper and mid ureter • Ureteroureterostomy • Trans ureteroureterostomy ( TUU) • Boari flap • Auto transplantation • Ileal Ureter • Distal ureter - Ureteroneocystostomy - Psoas hitch
Principles of Ureteral repair • Mobilise ureter – care on preserving adventitia • Debridement of nonviable tissue to a bleeding edge • Spatulated, tension free, water tight anastomosis