Download
1 / 44
440 likes | 657 Views
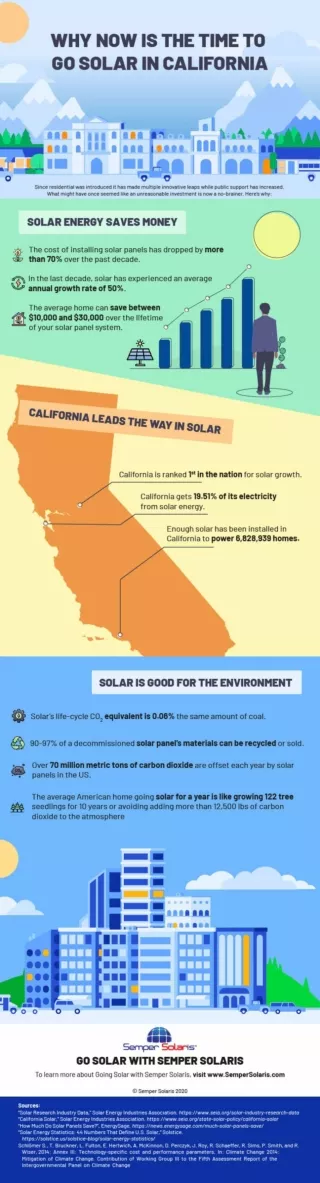
Why Now Is the Right Time to Work Together. Collaborative Family Healthcare Association 10 th Annual Conference Denver November 6, 2008. What We’ll Do This Evening.

E N D
Why Now Is the Right Time to Work Together Collaborative Family Healthcare Association 10th Annual Conference Denver November 6, 2008
What We’ll Do This Evening • We’ll review what we know about-- neuroscience, why we die prematurely, primary care, pertinent health professions workforce, and health care expenditures. • Do the assignment: i.e. Answer the question. • Plea for action now, using what we know.
40% Our behaviors 30% Our genetics 15% Our socioeconomic status 10% Shortfalls in medical care 5% Environment We Know Why We Die Prematurely
We Know • A person with a serious “mental health” problem, on average, dies 25 years sooner than other persons, at least in part because of a lack of clinical care. • A large portion of care for a person with mental health and/or substance use problems occurs in primary care settings, or not at all. • The US has a system of health care that emphasizes medical subspecialism in preference to primary care, public health, and mental health.
We Also Know: Primary Care Improves Population Health Outcomes • Generic outcomes are better in systems with stronger primary care (no study shows otherwise). • Primary care improves effectiveness. • Primary care improves efficiency. • Primary care improves equity.
Currently in Toxic Environment • No nationally recognized role in health care. • Insufficient technology. • Horrible business model. • Main effects compromise prevailing US paradigm of wealthcare. • Erosion of comprehensiveness. • Segregation of so-called mental and physical health.
Direct Patient Care Physicians (MD&DO) Population growth 1991-2006 = 19%
Primary Care Workforce Sept 2007 • 97,752 family physicians/general practitioners (1 for every 3, 081 persons; 14.4% of the physician workforce). • 92,257 general internists (1 per 2,443 adults) and 48,930 general pediatricians (1 for 1,548 children and adolescents). • 238,939 primary care physicians (1 for every 1,260 persons).
Nurse Practitioners and Physicians Assistants • The number of nurse practitioners grew 120% to 155,990 between 1996 and 2004. Upwards of 80% were practicing in primary care in 2000. • The number of physician assistants grew 160% between 1996 and 2007, to 69,473. Only one-third (34%) practice in primary care, down from half a decade earlier.
Psychologists • Of about 102,000 PhD psychologists, approximately 91,400 are employed, 70,300 or so full time. • 3% Annual growth rate in workforce. • APA estimates there are about 31,500 licensed clinical psychologists. • In 2006, there were about 3600 PhD’s awarded and about 1500 PsyD’s.
Psychiatrists • Around 1980 GMENAC estimated a need for 15.4 psychiatrists per 100,000 people. • In 2000 there were about 45,600 psychiatrists (about 39,400 adult) representing about 16.5/100,000. • The March 2008 psychiatry match resulted in 1013 psychiatry categorical residents.
Social Workers • More than 600,000 people hold a social work degree. • A masters in social work is the predominant degree for licensed social workers (79%). • Almost 50% of the National Association of Social Workers 2008 membership survey respondents identified mental health or health care as their primary area of practice.
WHEW!! There’s a lot of folks foraging in our landscape!
Health Care Spending • 16% of the US Economy BUT • From 2000 – 2005 healthcare devoured nearly 25% of our Economic Growth
Health Care Expenses Health Education Defense
Unadjusted Expenditures 2005 vs. 1970: • 26x’s expenditures for personal health care • 18x’s national health care expenditures per capita • 30x’s for physician services • 37x’s for prescription drugs • 51x’s for insurance admin and net cost While GDP increased 12x’s and population grew 41%
Health Care Spending • 2008 health spending (estimated) $2.39 trillion ($2,390,000,000,000) • $7,868 per person (2008 estimate) • Increased from $2000-$4600 from 1980-2000 • $421 billion increase over 2005 • Projected to reach $4.3 trillion by 2017, nearly 20% of the economy
And the Results? 1960: U.S. Infant mortality 13th (of 28 developed countries) Women's Life expectancy 15th Men's Life expectancy 20th 2005: U.S. Infant mortality 25th among 28 developed countries (just behind Hungary & Poland) Women's Life expectancy 7th Men's Life expectancy 9th 2008: “US falls further behind on infant mortality rates. Between 2000 and 2005, the US made only tiny gains, dropping to 29th globally, tied with Poland and Slovenia.”
Health Care Spending Healthcare’s major role has become Economic Engine
Annual Health Insurance Premiums and Household Income, 1996 to 2005(Robert Graham Center: Devoe et al)
So! What are we to do?
Dr. Margaret ChanDirector-General, WHO2008 World Health Assembly Address “When I took office last year, I called for a return to primary health care as an approach to strengthening health systems. My commitment has deepened.” “ If we want to reach the health-related Millennium Development Goals, we must return to the values, principles, and approaches of primary health care.”
Global Health Perspective: WHO 2008 on WHY Integrating Mental Health into Primary Care Is So Important • The burden of mental disorders is great. • Mental and physical health problems are interwoven. • The treatment gap for mental disorders is enormous. • Primary care for mental health enhances access, human rights, affordability, and effectiveness. • Primary care for mental health generates good health outcomes.
IOM 2006 • Overarching Recommendation 2. The aims, rules, and strategies for redesign set forth in Crossing the Quality Chasm should be applied throughout M/SU health care on a day-to-day operational basis, but tailored to reflect the characteristics that distinguish care for these problems and illnesses from general health care.
IOM 2006 • Recommendation 5-1. To make collaboration and coordination of patients’ M/SU health care services the norm, providers of the services should establish clinically effective linkages within their own organizations and between providers of mental health and substance-use treatment.
IOM 2006 • Recommendation 5-2. To facilitate the delivery of coordinated care by primary care, mental health, and substance-use treatment providers: Primary care and specialty M/SU health care providers should transition along a continuum of evidence-based coordination models from (1) formal agreements among mental, substance-use, and primary health care providers; to (2) case management of mental, substance-use, and primary health care; to (3) collocation of mental, substance-use, and primary health care services; and then to (4) delivery of mental, substance-use, and primary health care through clinically integrated practices of primary and M/SU care providers. [read #4 as, “Make room for mental health and substance use problems in the Person Centered Medical Home.”]
IOM 2006 • Recommendation 9-2. Federal and state agencies and private foundations should create health services research strategies and innovative approaches that address treatment effectiveness and quality improvement in usual settings of care delivery. To that end, they should develop new research and demonstration funding models that encourage local innovation, that include research designs in addition to randomized controlled trials, that are committed to partnerships between researchers and stakeholders, and that create a critical mass of interdisciplinary research partnerships involving usual settings of care.
Harris Poll: September 2008 • “A strong majority of self-identified registered voters want the next president to make health care reform a top priority and start working on it immediately after taking office.” • “Adding the patient-centered medical home model to either presidential candidate’s health care plan had a positive effect on the respondents’ support, with about half of U.S. adults indicating they would be more likely to support either plan if the PCMH model were included. Moreover, the survey found that for those respondents who expressed an opinion of support for the patient-centered medical home model, more than 75 percent would increase their support for the next U.S. president’s health care reform plan if it includes a patient-centered medical home.”
Best Practice Panelists at the Federal Partners Nov 18-19, 2008 Morehouse Conference • La Clinica de la Raza • Cherokee Health System • Fayette Companies • Intermountain Health Care • White River Junction VA Medical Center • Michigan Mental Health Center • Alaska South Central Foundation
Summary and Conclusion • There is an urgent need for ACTION. • There is compelling evidence to integrate the care of people with emotional and behavioral problems with the rest of clinical care. • The redesign of primary care is an unprecedented opportunity to work together. • We have a large, skilled workforce to deploy. • There is a lot of money in play, renewable annually. • We know enough about what to do to begin.
A Re-framing • We should speak of people with “emotional and behavioral issues that derive from brain problems.” • We should end the separate histories of mental and physical “diseases” and treatments. • We are positioned to seize, not the opportunity of a lifetime, but an opportunity of several centuries finally actionable. • It’s time to make room for mental health in the person centered medical home.
A Question to Consider: IS IT NOT TIME FOR A NATIONAL PROGRAM OF COMPARATIVE CASE STUDIES-- TO GUIDE THE WIDESPREAD REDESIGN OF CARE TO UNITE PRIMARY CARE, “MENTAL HEALTH,” AND PEOPLE WITH EMOTIONAL AND BEHAVIORAL PROBLEMS?
Why Now Is the Right Time to Work Together Because we are resource rich, empowered with new knowledge and technology. Because we have ideas that are ripe for testing and widespread implementation. Because none of us can make this transformative leap alone--we need each other! Because we lack evidence that this is a good time to wait, keep on doing what we are doing now. Because people with emotional and behavioral problems suffer needlessly and die before their time—because of our inaction. Because it is necessary, possible, timely, and—RIGHT!.
Of course, While an organism, and a system, will change to preserve itself, "It is not necessary to change. Survival is not mandatory.” -W. Edwards Deming