Download

1 / 20
200 likes | 369 Views
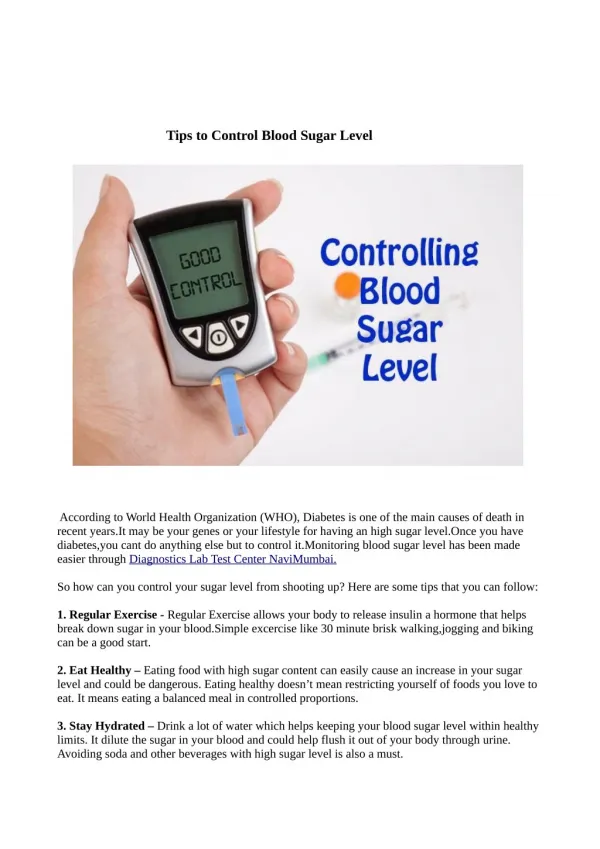
Sugar control in SICU. Ri 趙基安. Background. INTENSIVE INSULIN THERAPY IN CRITICALLY ILL PATIENTS The New England Journal of Medicine, volume 345, November 8, 2001,Number 19 ☆ Intensive insulin therapy: 80~110mg/dl ☆ Conventional therapy: insulin infusion starts when >215mg/dl

E N D
Sugar control in SICU Ri 趙基安
Background • INTENSIVE INSULIN THERAPY IN CRITICALLY ILL PATIENTS The New England Journal of Medicine, volume 345, November 8, 2001,Number 19 ☆ Intensive insulin therapy: 80~110mg/dl ☆ Conventional therapy: insulin infusion starts when >215mg/dl maintenance: 180~200mg/dl • Conclusion: reduces morbidity and mortality among critically ill patients in the surgical intensive care unit.
Outcome benefit of intensive insulin therapy in the critically ill: Insulin dose versus glycemic control, Critical Care Medicine, Volume 31(2),February 2003,pp 359-366 ☆ Conclusion: lowered blood glucose level was related to reduced mortality (p < .0001), critical illness polyneuropathy (p < .0001), bacteremia (p = .02), and inflammation (p = .0006) ☆ The prevention of acute renal failure: insulin dose was an independent determinant
Insulin protocol • van den Berghe G, et al.: BG control between 80~110mg/dL (4.4~6.1mmol/L) • Initial insulin infusion • Check BG Q1H
★Dose adjustment • blood glucose decreased by >50% the dose was reduced to half • blood glucose was 60~80 mg/dL insulin was reduced depending on the previous blood glucose level
blood glucose was 40~60 mg/dL stopped insulin infusion, gave adequate baseline glucose intake was given • blood glucose < 40 mg/dL stopped insulin infusion, adequate baseline glucose intake + glucose 10g intravenous boluses • blood glucose started to decrease within the normal range in a stable patient recovery of insulin sensitivity the insulin dose was reduced by 20%
☆ Factorsaffects insulin requirement • body mass index • history of diabetes • reason for intensive care unit admission • at-admission hyperglycemia • caloric intake • time in intensive care unit • Drugs affect insulin sensitivity ☆ Basal requirements: 0.01 U/kg/hr
Towards a feasible algorithm for tight glycemic control in critically ill patients: a systematic review of the literatureCritical Care 2006, 10:R19 • The goal set by van den Berghe G, et al is difficult to achieve in real-life ICU • Review 24 papers about blood glucose control
Conclusion: ☆ Set BG range between 4~8 mmol/L (72 to 144mg/dL) ☆ Continuous insulin infusion combined with frequent blood glucose determinations ☆ The use of the last two blood glucose values to determine the insulin infusion rate
Implementing intensive insulin therapy: Development and audit of the Bath insulin protocol Anaesthesia and Intensive care, volume 32, issue 3, 2004, p.311-316 • Not suitable for children, DKA and eating • Insulin should be started if blood glucose was greater than 7 mmol/L
An Insulin Infusion Protocol in Critically Ill Cardiothoracic Surgery Patients Annals of Pharmacotherapy 2004;38:1123-9. • Efficiently and significantly improved glycemic control in critically ill patients who underwent cardiothoracic surgery • No significantly increased the incidence of hypoglycemia
Introduction and evaluation of a computerised insulin protocol Intensive Care Med, 2007, 33:591–596 • Goal: 4.5~7.5 mmol/L • Exclusion: DKA, eat meals • Start insulin: single BG >9.0 mmol/L or second > 7.5mmol/L
☆ Advantages • Nurses only have to be trained to use the interface • Less chance of mistakes, since it is not necessary to read along lines or make calculations or comparisons by heart • Good compliance