Download
1 / 40
400 likes | 472 Views
Fractures - a violation of their integrity as a result of external mechanical factors or disease process. There diaphyseal (body bone), metaphyseal ( bilyasuhlobovi ) and epiphyseal ( vnutrisuhlobovi ) fractures. Changes in the joint during prolonged immobilization

E N D
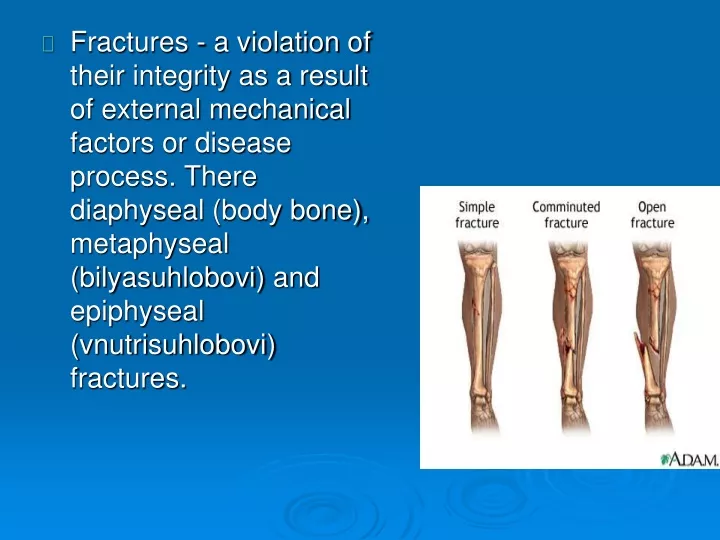
Fractures - a violation of their integrity as a result of external mechanical factors or disease process. There diaphyseal (body bone), metaphyseal (bilyasuhlobovi) and epiphyseal (vnutrisuhlobovi) fractures.
Changes in the joint during prolonged immobilization a - front cut normally functioning joint: 1, 2 - articular ends of the bones , 3 - articular cartilage, 4 - fibrous capsule ( outer layer ), 5 - subsynovialnyy intermediate layer , 6 - synovial membrane , 7 - joint space , 8 - lateral glenoid cavity b - front cut joints after prolonged immobilization : 1 - articular ends of the bones , 2 and 6 of the joint capsule that is wrinkled , 3 - articular cartilage , 4 - overgrown lateral articular cavity ( synovial membrane grows in areas it dublikatur ), 5 - glenoid cavity greatly reduced in volume , flows synovium on cartilage
. continuous use throughout the course of treatment, methods of exercise therapy varies depending on the treatment period; Early use of exercise, which provides not only improve the overall condition of the patient, but also prevents the occurrence of complications (pneumonia, contractures, atrophy); combination treatment with immobilization of exercise; gradual increase in capacity: moderation exercise intensity in the 1st period and intensification in the 3rd period; use of active and passive exercise Special methods:
Contraindications to exercise therapy appointment: - The general condition of the patient due to severe blood loss, trauma, infections, co-morbidities; - Fever, with the exception of long subfibrylnoyi (not above 37, 5 ); - The risk of occurrence or hemorrhage due to movement; - The presence of foreign bodies in the tissues located near major blood vessels, nerves and other vital organs; - The presence of other diseases that are contraindications to physical therapy appointment.
The period of immobilization. Lasts 30-90 days. Clinically characterized by acute effects of trauma, start the regenerative process in damaged tissues. Coincides with the formation of primary callus. In the absence of contraindications TE appointed since the early days of hospitalization. Common tasks: raising the general condition of the patient; improvement of vital systems: cardiovascular, respiratory, nervous, digestive, increase the body's resistance; prevent violations due to bed rest.
Special tasks: improvement trophic immobilized limb; consolidation of the fracture stimulation; prevention of muscle atrophy, joint dysfunction immobilized limb contractures and prevention tuhoruhomosti; develop the necessary temporary compensation. Forms of TE: therapeutic exercises, morning hygienic gymnastics, individual tasks for self-study.
- Normalize trophic injured limb (final formation of callus, the elimination of muscular atrophy); - To restore motion in joints damaged limbs; - Restore and normalize the function of the injured limb; - Restore correct posture, normalize motor skills, to improve their quality. Special tasks
Fig. 11 - Exercise for people with a fracture of the humerus (with S. Ivanov, 1970)
Special exercises for persons with injuries of the elbow joint and correction provisions (with AF Kaptyelinym, 1969): and - the movement to the polished panels; b - pokachuvannya at the elbow; in - motion using roller carts; r - bend at the elbow to support healthy hand; d - rolling stick, e - pokachuvannya sticks; same - laying hands between two bags of sand.
Exercise therapy for fractures of the spine. The course of physical therapy is divided into three periods (EF Drevynh): I - begins a few hours after the injury and immobilization and lasts for about 2 weeks; II - the next 2 weeks, ie until the end of the first month; III - In the 2nd month after the fracture.
- Increasing emotional state; - Promotion of the injured vertebrae in functional starting position; - Moderate toning the muscles of the back; - Improve circulation; - Prevention of pneumonia; - Activation of intestinal peristalsis. First time.Task:
The second period. Features physiotherapist: - Vigorous exercise for the muscles of the shoulder and pelvic girdle; - Inappropriate for pelvic girdle full load, so the movements are carried out each leg separately; - Training the back muscles - the extensor: not prescribe complex exercises and special exercises carried out not in full. The main principle of the classes - not painful movements. All movements of a busy performance facilitated inclined position of the bed.
Performed exercise, requiring good motor coordination and significant power voltage. Includes exercises to develop flexibility of the spine (lateral incline and rotation of the spine in longitudinal axis). To carry out strenuous bending of large amplitude and a burden. Third period.
Includes some navkarachky movements that increase flexibility of the spine, the end of the 2nd month - kneeling movements and movements with a small foothold.
Strengthening the patient. Improved circulation lesions of the body. Lowering elevated abnormal tone paretic muscles and increase muscle strength. Eliminating harmful spivdruzhnih movements: synergies and synkineses . Restoration of functional balance between paretic muscles and their synergists . Restore or improve the accuracy of movement. Recovery or improvement of nerve conduction from the center to the periphery and from the periphery to the center. Eliminating or weakening tremor of muscles. Play and forming the most important motor skills aimed at the development ( training) and labor skills, and self- movement , preparation for rehabilitation The task of physical therapy for diseases of the nervous system.
Features exercise therapy in neurological and neurosurgical disorders. • . Early administration of TE . Involve the use of stored functions and newly created , that are adapted to the changed conditions of neurological, visceral and somatic status. • Selective use of exercise therapy to restore disturbed functions or compensate for the lost . • Use special exercises by pathogenic principle in combination with general Firming effect of exercise therapy . • Respect for the principle of adequacy at a constant turnover of exercise , depending on the capabilities of the patient and the presence of a training effect. • Gradual expansion relentless motor mode from a prone position to unrestricted movement
Early administration of TE . Involve the use of stored functions and newly created , that are adapted to the changed conditions of neurological, visceral and somatic status. Selective use of exercise therapy to restore disturbed functions or compensate for the lost . Use special exercises by pathogenic principle in combination with general Firming effect of exercise therapy . Respect for the principle of adequacy at a constant turnover of exercise , depending on the capabilities of the patient and the presence of a training effect. Gradual expansion relentless motor mode from a prone position to unrestricted movement. Features exercise therapy in neurological and neurosurgical disorders.
By means of exercise therapy for diseases of the nervous system are assumptions, massage , special treatment and gymnastics . Latest share : a) to promote muscle strength ; b ) for the dosed muscular tension ; c) to obtain the differential stresses and relaxations of individual muscles and muscle groups; d) the right to play in the whole motor act (speed, smoothness , precision movements) ; e) protyataktychni exercises aimed at restoring and improving coordination ; e) antyspastychni and protyryhidni ; g) and ideomotor reflex ; i) the restoration or new formation of applied motor skills ( standing , walking , living skills ); c) Passive including manipulation .
Acute cerebrovascular accident - a stroke.. There are 3 stages of rehabilitation of stroke : 1st - early recovery ( up to 3 months) 2nd - late recovery (up to 1 year) 3rd - residual disturbances of motor functions. Degree of impairment of motor functions : 1st - light paresis ; 2nd - moderate paresis ; 3rd - paresis ; 4th - deep paresis ; 5th - plehiya or paralysis. Daily motor activity depends on: 1 - the patient's condition ; 2 - the period of the disease; 3 - stupernyu violations of motor functions. Modes of motion activity are: 1. Cots' severe (1-3 days). 2. 2nd Advanced bed (3-15 days). 2-B - 16-21 days. 3. Ward . 4. Available .
1. Treating the supine position on the side. 2. Exercise: - Breathing exercises; - Active exercises for small, medium, and later for large joints healthy limbs; 3. With a 3-6 day - passive exercises for the joints paretic limb. 4. Teach a determined reference pulses synchronized to the movements of the isolated passive extension of the forearm, flexion of the lower leg. Tools:
Objectives of TE: Increased general tonic effect on the patient. Learning relaxation of muscles healthy limb. Decreased muscle tone in the paretic limbs. Transfer the patient in a sitting position. Stimulation of active movements in the paretic limbs. Combating pathological synkineziyam. Preparing the patient for ambulation. Restoration tool support in the lower extremities. Restoring function self healthy limb. Extended bed rest: 2b / 16-21 days.
Tools: 1. Assumptions - are important in the implementation of passive movements of individual segments of the limbs : Fingers unbend easily if bent tassel . Forearm - arm if given. Supination of the forearm is complete when the elbow is bent . Pleas hip - fuller in a bent position. 2. a) classes begin the active exercise for healthy limbs first , then passive - paralytic . b ) during active exercise is necessary to use lightweight provision using: - Bed frame; - Blocks ; - Hamachky to maintain paralytic limbs ; c) exercises performed slowly, slowly , every movement 4-8 times. First limb returns to the starting position passively , through the instructor and support. Particular attention is paid to the recovery movement 1 - the first finger ;
d) passively or actively oppose pathological synkineziyam: - During the execution of active movements of foot hands fixed behind head or across the body, brush under the buttocks; - When healthy arm bent, Methodist can at this time passively straighten paretic hand; - Use willpower, bending the leg the patient prevents bending arm, holding it in an effort to straighten position; e) ideomotor movements; e) isometric muscle tension paretic limb.
Objectives of TE: Decreased muscle tone. Combating hemiplehichnym contractures. Further recovery of active movements. Switching to a standing position. Learning to walk. Combating synkineziyam. Restoration and applied skills of self-domestic movements. ward mode
Free mode . Objective means and methods of exercise therapy in late stage restorative and during the remaining movement disorders depends on the disturbances of motor functions : 1st degree (mild paresis ) - General tonic effect on the body ; - Strengthening the muscles of the shoulder girdle and back; - Improve posture; - Travel, walking. 5th degree ( plehiya , paralysis ) - Activation of the cardiovascular and respiratory systems; - Training the patient to return to the side ; - Preparing to move into a sitting position or standing ; - Better support of the lower extremities; - Relaxation of the muscles of healthy limbs; - Decrease in muscle tone ; - Anti contractures ; - Violation of trophic paretic extremities; - Expanding the skills of self .
Exercise therapy in paralysis and paresis. Paralysis (Greek paralysis) - loss, paresis (Greek haresis) - 1) attenuation of motor function with no or decreased muscle strength, and 2) because of a violation of the structure and function of the motor analyzer, and 3) as a result of pathological processes in the nervous system. Shared by such forms of paralysis and paresis: The nature of the damage and the violation of the relevant structures of the nervous system:
The nature of the affected muscle tone distinguished: central or spastic, flabby (peripheral) and rigid paralysis and paresis. Depending on the level of structural lesions of the motor analyzer paralysis and paresis divided into:
Objectives of gymnastics in the central and peripheral paralysis. • . Improved blood flow and nerve trophic lesions of muscles. • Prevention of contractures. • Restoration of movement and development of compensatory motor skills. • General-firming effect on the patient's
Use the treatment position, massage, medical gymnastics. Treatment provision: sleep on the side (on the affected side); during the day, 3-4 times to sit, head bent in the opposite direction, keeping her hand on elbow with resistance. At the same time tighten the muscles of the healthy side to side lesions (bottom to top) tries to restore the symmetry of the face; leykoplasternyy tension with the healthy side in patients using a special helmet mask; tying a handkerchief; The early period
1. Raise your eyebrows upwards. 2. Nahmuryty eyebrows. 3. Close Your Eyes (phases of the exercise: look down, close your eyes, holding the eyelid with your fingers on the side of injury, keep your eyes closed for a minute, close your eyes and open 3 times). 4. Smile with your mouth closed. 5. Schurytysya. 6. Lower your head down, take a breath and exhale during the "snort". 7. Whistle. 8. Expand nostrils. 9. Lift the upper lip, upper teeth show. 10. Lowering the lower lip, the lower teeth show. 11. Smile with your mouth open. 12. Redeem a match. Special exercises for facial muscles:
13. A mouthful of water, and rinse your mouth shut , not pouring water. 14. Inflate cheeks. 15. Move air from the mouth of one half to the other. 16. Lower down the corners of his mouth with a closed mouth. 17. Protruding tongue and make it narrower. 18. Move the tongue forward - back with open mouth. 19. Move your tongue right - left with an open mouth. 20. Outstretched lips " tube ". 21. Finger make a circle , watching him eyes. 22. Retract the cheek with a closed mouth. 23. Lower the upper lip to the bottom . 24. In the closed mouth to drive the tip of the tongue on the Desna left or right, tongue pressing various efforts.
13. A mouthful of water, and rinse your mouth shut , not pouring water. 14. Inflate cheeks. 15. Move air from the mouth of one half to the other. 16. Lower down the corners of his mouth with a closed mouth. 17. Protruding tongue and make it narrower. 18. Move the tongue forward - back with open mouth. 19. Move your tongue right - left with an open mouth. 20. Outstretched lips " tube ". 21. Finger make a circle , watching him eyes. 22. Retract the cheek with a closed mouth. 23. Lower the upper lip to the bottom . 24. In the closed mouth to drive the tip of the tongue on the Desna left or right, tongue pressing various efforts.
Exercise therapy in spinal osteochondrosis . At the heart of spinal osteochondrosis is changing intervertebral disc with subsequent involvement in the process of vertebral bodies adjacent intervertebral joints and ligaments . Intervertebral discs play an important role in the stable position of the vertebrae , provide mobility of the spine, act as biological shock absorber. Factors that contribute to the emergence and development of osteochondrosis is a sedentary lifestyle , prolonged exposure of the body physiologically in an awkward position ( many hours sitting at a desk, driving a car , standing next to the machine, behind the counter ). This greatly impairs blood circulation and providing nutrients to the vertebral bodies , intervertebral discs. There are cracks fibrous ring . Due to the progression of degenerative changes in the fibrous ring fixing broken vertebrae together , there is abnormal mobility . Intervertebral gap reduced, compressed neurovascular end , blood and lymph vessels - amplified pain. In the 3rd stage of the disease there is a rupture of the annulus fibrosus , intervertebral hernia formation . The final stage is characterized by a painful thickening and displacement of the vertebrae, the formation of abnormal bone growths .
The task of the physiotherapist : Help to increase the distance between individual vertebral segments to relieve pathological proprioceptive impulses. Help to reduce pathological proprioceptive impulses. Improving metabolism due to increased blood and lymph circulation in the damaged vertebral segment and roots. Reduce swelling in the tissues located in the region of the intervertebral foramen, improve blood circulation in the affected limb . Increasing and restoring full range of motion in the extremities and spine , reducing static and dynamic disturbances and compensatory movements, restoration of impaired posture . Help restore trophic, tone, muscle strength of the trunk and extremities. Improve overall physical performance.
Special task gymnastics: When radicular syndrome: stretching of nerve trunks and roots; prevention of muscle atrophy; strengthening muscles distal extremities. When glenohumeralperyartryti: prevention of the formation of neurogenic reflex contracture of the elbow joint; strengthening the deltoid, nadostnoho, pidostnoho, the biceps muscle. In the posterior cervical pretty syndrome (vertebral artery syndrome): contribute to the weakening of vestibular disorders.
Osteochondrosis of the cervical spine. Active movement of the cervical spine in the initial and main periods of treatment are contraindicated, as it can cause narrowing of the intervertebral foramen, which cause compression of the nerve roots and blood vessels.
Fig. 16 - Exercise for the flexibility of the spine (set of 4) and upper shoulder girdle (set of 5).
Complex 6 Fig. 17 - Exercise for the muscles of the lower back and abdominals.