Download
1 / 13
130 likes | 206 Views
Jim.r.dudl@gmail.com Diabetes Lead Care Management Institute, Kaiser Permanente. Should YOU Implement ALL? Or Use It As Step 1 of Titration to BP & Lipid Targets?. What Works for CVD Prevention?. Evidence for ALL [ A spirin, L isinopril & L ipid lowering] in Pts with CVD or DM >55yo

E N D
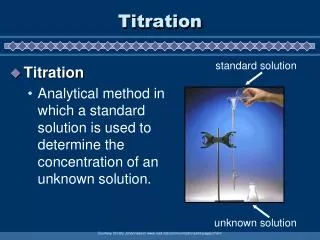
Jim.r.dudl@gmail.com Diabetes Lead Care Management Institute, Kaiser Permanente Should YOU Implement ALL?Or Use It As Step 1 of Titration to BP & Lipid Targets?
What Works for CVD Prevention? Evidence for ALL [Aspirin, Lisinopril & Lipid lowering] in Pts with CVD or DM >55yo Archimedes modeled a 71% drop in CVD events & >$300/pt/yr savings In an observational study* “LL” was able to be implemented in ~70,000 pts in California Kaiser in 2 years in the 3rd year after starting LL, there were found to be 1,271 fewer strokes & MI’s than in the group w/o the bundle, [>60% decrease] Other literature regarding “fixed dose” benefit: In STENO 2 the combined use of lipid lowering, ACEI use and aspirin with other therapies achieved >59% drop in CVD deaths and higher decrease in events** Is this the best POSSIBLE evidence? No, but look at the alternatives: **N Engl J Med 2008 358 580 *Am J Manag Care. 2009;15(10):e88-e94)
What Works for CVD Prevention? Support for Treat to Target by ADA & AHA: LDLc <100 with 30+% fewer MI & strokes if mid strength/dose statin used & SBP<140/90 targets & [<130/80 in DM?] with benefit of control documented to save CVD events & lives in UKPDS, better than glucose control did. What’s still questionable? Targets! NCQA is considering either achieving the target LDL OR being on a statin Not using BP 130/80 in DM ASA in DM: but ADA & AHA still recommend 50yo male 60yo female be considered for it. *Am J Manag Care. 2009;15(10):e88-e94)
Opportunity Cost of Waiting for the“Best Possible” Evidence What’s tragic is not starting treatments known to work: Lots of people with CVD or DM and are over lipid goal and not on a statin, or over BP goal and not on an ACEI, missing the benefits. What do we agree on? Evidence for if LDLc is over 80 simvastatin 40 mg was shown to drop MI’s 33%* >55yo DM pts with mean BP 133 mm hg syst, an ACEI decreased cvd 22%** As the Institute of Medicine has concluded, in many areas, we need to “recommend strategies based on the best available evidence as opposed to waiting for the best possible evidence”*** So why don’t we consider “[A]LL as therapy, or if not, at least step 1 of treating to target? * Lancet 2003 361 529-53 **Lancet 2000 355 253-59 ***http://www.iom.edu/CMS/3788/25044/34007.aspx
Why Start With ALL NOW? “Implementability”! “LL” has been implemented in 2 yrs in ~70,000 Californians in Kaiser It is simpler, cheaper, and more convenient than Treat to target Similar characteristics to disruptive innovation* This may open use to those previously not treated due to cost, titration visits and laboratory tests. It is simple enough providers can focus on patient barriers to initiation, titration and adherence, 55% of reasons treatments are not effective** *C Christiansen, Health Affairs 27, no. 5 (2007):1329–1335 **Am J Gen Med
Keys to Large Scale Implementation: Strong management that funds and is supportive of implementation changes Simplicity: no need to focus on algorithm Fix accountability, then monthly quality Improvement meetings FOCUSED exactly the 1-2 metrics you want to improve Training practitioners on TIA [Titration Initiation Adherence] with focus on helping patients remove barriers
Simplicity: Focus on 1 Step ALL implementation: essentially 1 step with three drugs. TIA behavioral focus on removing pt barriers. Or LDLc<100: simvastatin 40-80 mg BP>140:Focus on Prinzide
Would Simvastatin Work? Simvastatin: 40 – 80 mg initiation/titration Simvastatin opportunity: No stain: ~10% or more Less than 40 mg [of all but ceruvostatin]: 10% Would that lower it enough: most <60 mg% to go 50% less than 30 mg% to target 75% less than 60 mg% to target What works for lack of adherence? One pharmacist call 40% picked up a prescription
Would Prinzide/Amlodipine Work? Would adding 1-2 meds work?
How Many DRUG Class’ Does It Take to Control BP in DM: UKPDS ~70% ACCORD: <140 2.1 drugs/pers, <120 3.4 drugs per person BMJ 1998;317;703-713 10
Are There Enough Patients Not on Them to Increase 10% Control? Prinzide opportunity >30% Not on prinzide >20% Not on max dose <10% Is it strong enough: Majority of pts are <10 mm Hg systolic away Over 75% 20 mm, prinzide/amlodipine range Can it be done: Inside Kaiser one region 5,000 pts with significant drop in BP correlated with use
Summary & Conclusions:Either-Or? Measuring effect may dictate use of: ALL: if measuring med fills/refills or staff education not a barrier, it’s the cheapest/simplest/easiest path. BP/LDLc: if HEIDS is dominant or culture demands hitting targets, this can be used Which is best? Consider starting with [A]LL, then increase if you wish to treat to target
Questions? Contact Information: Jim.r.dudl@kp.org 858 459 4743 [O/H] 858 220 1012 [c]