Download
1 / 19
190 likes | 316 Views
ANTENATAL CORTICOSTEROID USE IN PRETERM DELIVERY AT K ENYATTA N ATIONAL H OSPITAL. PRINCIPAL INVESTIGATOR: DR . GWAKO G. N SUPERVISORS: PROF. QURESHI Z.N; DR. KUDOYI W.O; PROF. WERE F . KNH/UON MNCH SYMPOSIUM UON LT3 10-Jan-2013. Introduction.

E N D
ANTENATAL CORTICOSTEROID USE IN PRETERM DELIVERY AT KENYATTA NATIONAL HOSPITAL PRINCIPAL INVESTIGATOR:DR. GWAKO G. N SUPERVISORS: PROF. QURESHI Z.N; DR. KUDOYI W.O; PROF. WERE F. KNH/UON MNCH SYMPOSIUM UON LT3 10-Jan-2013
Introduction • PRETERM birth causes ≥75% of neonatal deaths that are not attributable to congenital malformations. • ACS given to mothers at risk of preterm birth reduce the incidence and severity of RDS, IVH, NEC and neonatal deaths. • WHO recommends the use of one course of ACS for all pregnant women between 26 and 35wks who are at risk of preterm delivery within 7 days. ACOG and RCOG recommend their use between 24 and 34 weeks of gestation. • The use of ACS after 34 or 35 weeks of gestation is not recommended.
Objectives • To determine the: • frequency of adminstrationof ACS • impact of ACS in reducing the incidence and severity of RDS; NBU admissions and neonatal deaths in preterm neonates (28- 37 weeks gestation), born to women with PTL, PPROM or severe preeclampsia at KNH.
Methods • Site: Kenyatta National Hospital. Study design: cross sectional • Study population: mothers with preterm birth between 28-37 weeks gestation and their neonates. • Methodology: women who met the inclusion criteria and consented for the study were recruited sequentially immediately after delivery. Interviews. Medical records. Neonates followed up until discharge/death or the 7th day. • Outcome measures: occurrence of RDS, severity of RDS,NBU/NICU admissions and neonatal deaths
Summary Results • A total of 206 mother/neonate pairs were recruited. • 114(55.4%) mothers had spontaneous preterm labour, 53(25.1%) had PPROM, 39(18.9%) had severe pre-eclampsia. • 72(34.9%) mothers received antenatal steroids: • 46 % of those who delivered before 34weeks • 26% of those who delivered after 34 weeks
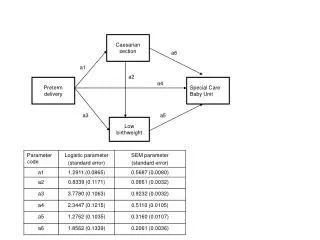
Impact of ACS on occurrence of RDS: • Any number of ACS doses, any interval between first dose and delivery(n=206)
….delivery after 48hrs of ACS exposure vs no exposure(n=147)
Impact of ACS use on oxygen therapy • Need for oxygen therapy(n=201)
Impact of ACS use on NBU and NICU admissions • ….NBU admissions(n=198)
Conclusions • Exposure to antenatal steroids reduces the incidence and severity of respiratory distress syndrome and neonatal mortality. This reduction is however more significant in those neonates delivered before 34 weeks of gestation.
Recommendations • This study shows that there is no extra benefit of ACS use after 34 weeks gestation; clinicians should to be sensitized on need to avoid their unnecessary use after this gestation. • During the course of the study it was noted there was no SOP at KNH on use of ACS in terms of which steroids to use, dosage and number of courses to be administered. It will be important for KNH to develop such a protocol. • ACS are effective and yet underutilized.