Download
1 / 24
250 likes | 937 Views
Diverticulitis-an update. Dr Bernard Stacey Consultant Gastroenterologist SUHT. Aims. The natural history of diverticular disease Medical treatment for the majority of patients with diverticular disease? Who needs surgery? Is age a problem?

E N D
Diverticulitis-an update Dr Bernard Stacey Consultant Gastroenterologist SUHT
Aims • The natural history of diverticular disease • Medical treatment for the majority of patients with diverticular disease? • Who needs surgery? • Is age a problem? • What about patients with chronic LIF pain and associated diverticular disease?
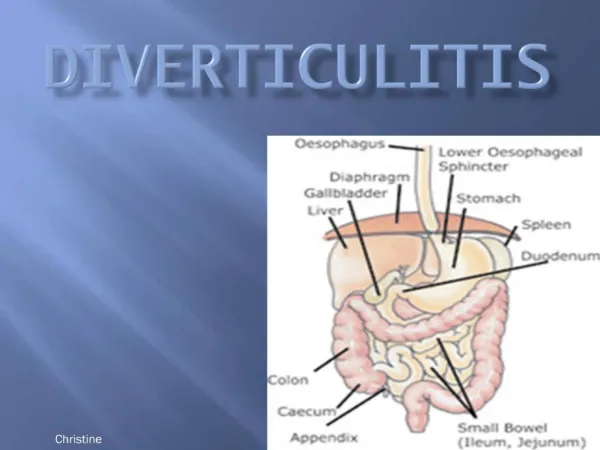
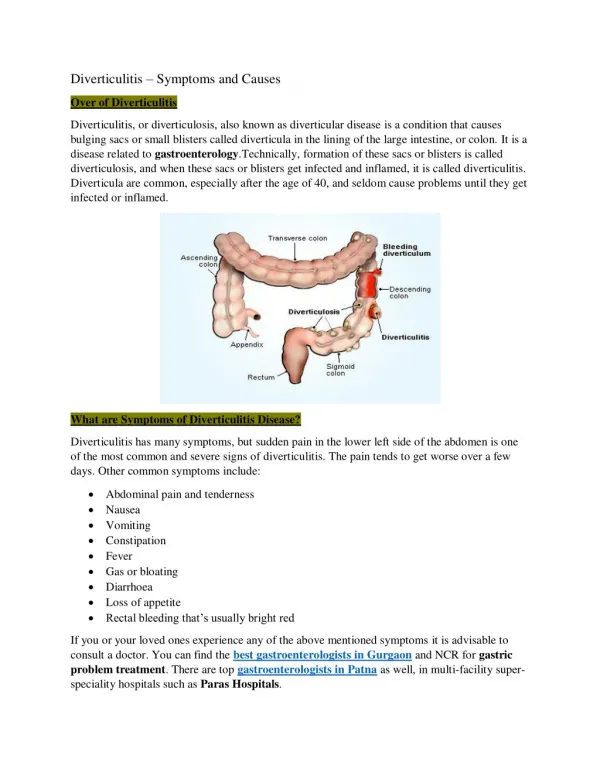
Colonic diverticula are mucosal outpouchings through the large bowel wall Often accompanied by structural changes (elastosis of the taenia coli, muscular thickening, and mucosal folding) Usually multiple Most frequently in the sigmoid colon Diverticulae
Geography/Diet • Diverticulosis is common in resource-rich countries • There is a lower prevalence of diverticulosis in Western vegetarians consuming a diet high in fibre • Diverticulosis is almost unknown in rural Africa and Asia
Spectrum of presentation • Majority of people with colonic diverticula are asymptomatic = Diverticulosis • 20% develop symptoms at some point = Diverticular disease • When diverticulum becomes acutely inflamed =Acute diverticulitis
Complex Colonic Diverticular Disease Jacobs D. N Engl J Med 2007;357:2057-2066
Complications • Complications of diverticular disease • perforation • obstruction • haemorrhage • fistula formation are each seen in about 5% of people with colonic diverticula when followed up for 10–30 years • UK incidence of perforation is 4 cases/100,000 people a year, leading to approximately 2000 cases annually
Prevalence of Diverticulosis • 5% to 10% before age 50 • 30% after age of 50 • 50% over age70 • 66% over age 85 Natural history of diverticular disease of the colonParks TG
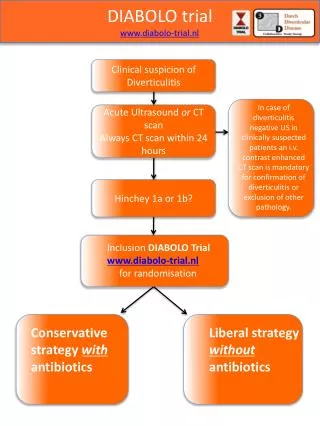
Hinchey Classification Scheme Hinchey 1 - peri-diverticular abscess within the mesocolon Hinchey II - distant (pelvic, retroperitoneal) abscess Hinchey III - generalized purulent peritonitis Hinchey IV – generalised faecal peritonitis Jacobs D. N Engl J Med 2007;357:2057-2066
How to treat? • If can tolerate fluids and have no peritonitis • Fluids or Low residue liquid diet • Pain relief • Antibiotics (7-10 days) of oral broad spectrum antimicrobial therapy – ciprofloxacin and metronidazole • Need imaging of bowel to exclude other pathology (10%) • Management can be repeated • Consider hospital if unable to tolerate fluids, cannot manage pain, fails to improve or has complicated diverticulitis
Acute hospital admission • Drip (+/- suck) • IV antibiotics • CT • high sensitivity – 93-97% • specificity – 100% • Barium enema / colonoscopy / flex sig to check for other pathology (avoid for 6 weeks)
CT Scans of the Colon in Four Patients with Diverticulitis of Varying Severity
Who needs operation? • Hinchey I - conservative • Hinchey II distal or large abscess > 4cm: CT drainage • Less than 10% of Hinchey I and II need operation • Hinchey III – usually operation • Hinchey IV – always operation
Outcome at presentation– Hinchey stage Risk of death: • <5% for most patients with stage 1 or 2 • 13 % for stage 3 • 43% for stage 4
Does one or more attacks predict further or more serious ones? NO • >50% of patients presenting to hospital with complicated diverticular disease - first presentation • 70% of these will have perforation
What happens after first attack? • Recurrent diverticulitis is observed in 7–42% • 2551 patients followed up over 9 years – 13% recurrent attacks and 7% required surgery • 10% recurrence in 1st year and 3% each year afterwards
Medical treatment • Fibre • Lancet 1977 Broadribb • 18 patients single randomised controlled trial with crossover. Stopped at 3 months • Caused a reduction in symptoms! • Probiotics • 2 small trials • Longer remission • 5ASA • 3 trials • Reduce peridiverticular inflammation
Disease progression • Inflammation will develop in 10–25% of people with diverticula at some point • Even after successful medical treatment of acute diverticulitis, almost two thirds of people suffer recurrent pain in the lower abdomen
Spectrum of symptoms with IBS • People with uncomplicated diverticular disease may report • abdominal pain (principally colicky left iliac fossa pain) • bloating • altered bowel habit • may have mild left iliac fossa tenderness on examination.
To operate or not? • Decreasing morbidity and mortality with laparoscopic colonic surgery • Some cases of chronic pain and recurrent attacks do extremely well • Need to ‘earn’ their surgery and understand the risks
Summary • Most people in the Western World will develop diverticulae • Most will remain asymptomatic • The most serious complication is faecal perforation (43% mortality) – most likely to occur at first attack • After first attack of complicated diverticulitis 10% recur in the first year – then 3% per year
Summary • If can tolerate fluids • Treat at home with fluids, antibiotics for 7-10 days and then put on fybogel, probiotics and ?ASA • If cannot manage pain relief or fluids, or patient sick admit • 2 attacks no longer means surgery • Tailor on-going management plan according to patient needs
Conclusion • Perforated diverticulitis kills but we cannot predict the group in whom this occurs • Surgery kills – must think carefully before doing surgery