Download
1 / 14
150 likes | 429 Views
The Effect of Celecoxib, a Cyclooxegenase-2 Inhibitor, In Familial Adenematous Polyposis.

E N D
The Effect of Celecoxib, a Cyclooxegenase-2 Inhibitor, In Familial Adenematous Polyposis Gideon Steinbach, M.D., Ph. D., Patrick Lynch, M.D., J.D., Robin K.S. Phillips, M.B., B.S., Marina H. Wallace, M.B., B.S., Ernest Hawk, M.D., M.P.H., Gary B. Gordon, M.D., Ph.D., Naoki Wakabayashi, M.D., Ph.D., Brian Saunders, M.D., Yu Shien, Ph.D., Takashi Fujimara, M.D., Li-Kuo Su, Ph.D., and Bernard Levin, M.D.
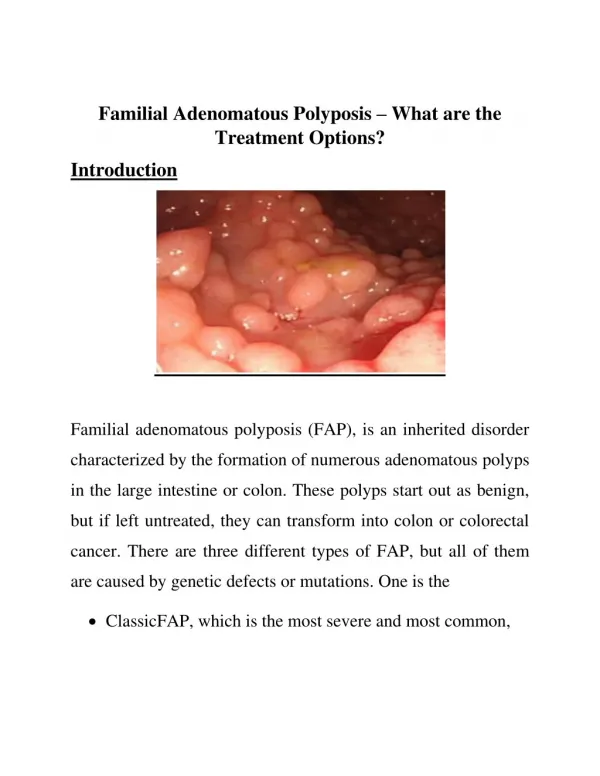
Why Familial Adenomatous Polyposis? • Human colon cancer develops from normal mucosa to adenomatous polyps to carcinoma • Patients with FAP as a result of germ-line mutations in the Adenomatous Polyposis Coli gene have a nearly 100 % risk of colon cancer • Study of FAP may provide insight helpful for sporadic adenomas that develop as a result of mutations in the APC gene
Cyclooxegenase-2 and Colon Cancer • Cox-2 derived prostoglandins may interact with malignant epithelial cells (cell-autonomous) or surrounding stromal cells (landscaping effect) • Cell-autonomous effects: changes in key regulatory genes that inhibit apoptosis and enhance migration • Landscaping effects: Cox-2 supports fibroblast neurovascularization near tumors Gupta, RA, and Dubois, RN. Colorectal Cancer Prevention and Treatment by Inhibition of Cyclooxegenase-2. Nature Reviews: Cancer. Oct., 2001 (1): 11-23.
Sulindac and Rectal Adenomas • Sulindac, a nonselective cyclooxeganase inhibitor, caused regression in controlled and uncontrolled studies • Rapid recurrence observed after discontinuing therapy (~3-4 mo) • But, sulindac was found to inhibit normal COX-1 activities, leading to gastric ulceration
Study Design • Double-Blind Study • Placebo Controlled • Age Discrepancy? • Surgical Status?
Celecoxib Efficacy • 400 mg Celecoxib treatment 2x daily is most effective in reducing total number of polyps • 400 mg Celecoxib treatment 2x daily was most effective in reducing total polyp burden (average sum of polyp diameters) • Regression in patients given the Placebo?
Distribution of Polyp Regression • Patients receiving Celecoxib treatment (100 or 400 mg) show definite bias towards reduction in number of polyps • Large outlyer population in these groups?
Change in Colorectal Polyposis • Patients receiving 400 mg of Celecoxib 2x daily show improvement in all areas of colon • Patients receiving 100 mg of Celecoxib 2x daily show trend towards improvement in rectum, ascending colon, and cecum • Are these two areas the first targets of cox-2 inhibitor-mediated polyp regression? Is the mechanism different for different dosages?
Side Effects? • Most common adverse events reported were diarrhea and abdominal pain • Incidence of each event was similar among all groups: diarrhea (placebo, 13%, 400mg 2x daily, 13 %, and 100 mg 2x daily, 19%) and abdominal pain (placebo, 13%, 400mg 2x daily, 3 %, and 100 mg 2x daily, 7%)
Is This Really Cox-2 Inhibition? • High Doses of NSAIDs (50-1000 um) can induce apoptosis in vitro independently of COX-2 (or COX-1) by: • Inhibition of IKKBeta Kinase • Decreasing the levels of anti-apoptosis protein BCL-X • Overexpressing pro-apoptitic (?) Peroxisome Proliferator Activated Receptor • What is bioavailable in Celecoxib Treatment?
What Now? • Study the role of COX-2 inhibition in prevention of adenoma development in pre-clinical FAP adolescents • Study the role of COX-2 inhibition in the prevention of colorectal tumors in persons with sporadic adenomatous polyps
Can COX-2 Inhibitors Prevent Polyp Formation? Giardello, FM, et. Al. Primary Chemoprevention of Familial Adenomatous Polyposis with Sulindac. N Eng J Med 2002 (346): 1054-9. • Clinical trials in 2002 with Sulindac (non-specific COX inhibtion) in 41 young patients with FAP genotype who were phenotypically unaffected • Prostoglandin production in the mucosa was lower than in the placebo group • However, “standard doses of sulindac did not prevent the development of adenomas in subjects with FAP” (NEJM, 2002; 346:1054-9)
Treatment Issues • COX-2 inhibition of development of sporadic colon cancer? • Inhibition of Microsatellite unstable tumorigenesis • Treatment of colorectal cancer in the context of Inflammatory Bowel Disease?