Download
1 / 30
320 likes | 507 Views
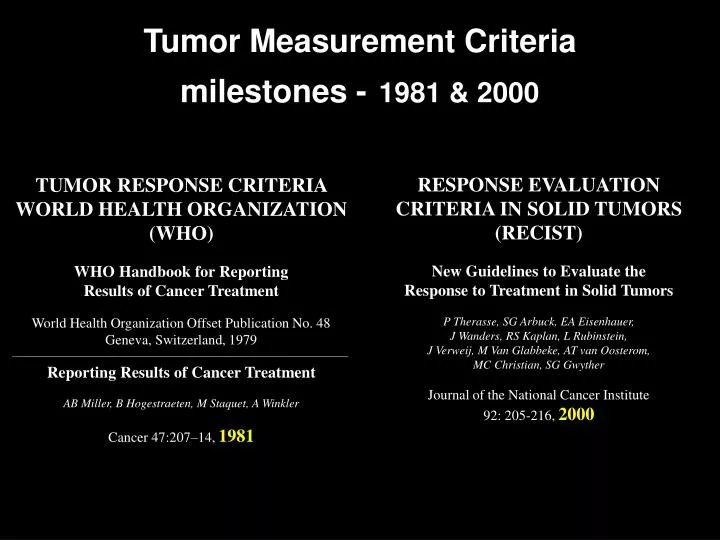
Tumor Measurement Criteria milestones - 1981 & 2000. RESPONSE EVALUATION CRITERIA IN SOLID TUMORS (RECIST) New Guidelines to Evaluate the Response to Treatment in Solid Tumors

E N D
Tumor Measurement Criteriamilestones -1981 & 2000 RESPONSE EVALUATION CRITERIA IN SOLID TUMORS (RECIST) New Guidelines to Evaluate the Response to Treatment in Solid Tumors P Therasse, SG Arbuck, EA Eisenhauer,J Wanders, RS Kaplan, L Rubinstein, J Verweij, M Van Glabbeke, AT van Oosterom, MC Christian, SG Gwyther Journal of the National Cancer Institute 92: 205-216, 2000 TUMOR RESPONSE CRITERIA WORLD HEALTH ORGANIZATION(WHO) WHO Handbook for Reporting Results of Cancer Treatment World Health Organization Offset Publication No. 48Geneva, Switzerland, 1979 ———————————————————————————— Reporting Results of Cancer Treatment AB Miller, B Hogestraeten, M Staquet, A Winkler Cancer 47:207–14, 1981
WHO bi-linear measurement Baseline 8 Weeks
RECIST CriteriaResponse Evaluation Criteria In Solid Tumors Simplification of former methods 4 response categories (CR, PR, PD, SD) Based on linear 1-D being as good as 2-D Least effort, conservative, for widest acceptance
RECIST Criteria • CR = disappearance of all target lesions • PR = 30% decrease in the sum of the longest diameter of target lesions • PD = 20% increase in the sum of the longest diameter of target lesions • SD = small changes that don’t meet above criteria CR = complete response PR = partial response PD = progressive disease SD = stable disease
RECIST criteria ‘Target’ lesions • All measurable lesions up to a maximum of five lesions per organ, and 10 lesions in total • Sum of the longest diameter of all of the target lesions
RECIST • RECIST criteria may be employed by NCI-funded cooperative groups which are encouraged, but not required, to use • RECIST criteria are a voluntary, international standard, and not an NCI standard • That doesn’t mean Clinical Trial groups are satisfied with it
baseline 20 weeks (PR at - 39%) 24 weeks (PR confirmed - 52%) 52 weeks (- 74%) metastatic renal cell
baseline 13 wks (– 7 %) 27 wks (PR – 43 %) metastatic renal cell
The Value of Image Data Validated image data could lead to: • Smaller clinical trials with fewer patients • Earlier go/no decisions on compounds • Faster regulatory approval • Shorter time to market
Biomarker • a measurable characteristic that predicts a clinical endpoint • “surrogate marker” is a biomarker that substitutes for a clinical endpoint • “surrogate marker” is a special case biomarker, i.e, not just a predictor of a clinical endpoint, but a reliable substitute for a clinical endpoint • the distinction has regulatory implications • Outcome data is needed to establish validity of a surrogate marker
First steps • Appropriate, disease-sensitive imaging • Uniformly acquired with objective QA • Quantitatively assessed • Centrally accessible with metadata
Lung nodule volume growth Time Difference = 130 days linear dimension increased 8 mm -> 11 mm in 4 months A.P.Reeves, Cornell University, 1999
Why not calculate volumes? • No fully automatic, objective methods • Semi-automatic methods are time-consuming, labor-intensive, and/or not user-friendly.
“Non-cytoreductive”(i.e. functional) measures • FDG-PET • DCE-MRI • MR spectroscopy • CT density and contrast dynamics • Future: • Other PET ligands • Macromolecular MR agents • Optical methods
PET, CT, hybrid PET/CT forGIST response to imatinib (Gleevec) baseline 7 wks post rx G. W. Goerres et al, Univ Hosp Zurich
Visual: subjectiveStandardized Uptake Value (SUV): semi-quantitativeKinetic analysis: quantitative Concerns about assessing 18FDG uptake in malignant tissue:
DCE MRI VEGF Inhibition time after contrast bolus (PTK/ZK TK inhibitor oral dose results on colon mets) Morgan B et al, JCO 2003
Chemotherapy Response by MRI & MRS 1 wk pre-Tx 76 cc Day 1 AC x1 79 cc Day 42 AC x3 26 cc Day 70 AC x4 25 cc Day 112 taxol x2 11 cc Day 178 taxol x4 6 cc 486 593 267 79 481 595 partial response to AC, regrowth on taxol final pathology - viable IDC and extensive DCIS Univ. of Minnesota
NCI-FDA Interagency Oncology Task Force • Imaging Science Development for Oncologic Applications – Work in Progress • Develop volumetric anatomical imaging for oncology e.g. revise (RECIST) • Develop standard dynamic (contrast) imaging techniques for oncologic drug development and as surrogate endpoint for drug approvals • Validate FDG-PET for oncologic drug development and as a surrogate endpoint for drug approvals • Develop a pathway for accelerating molecular imaging including ‘first in human’ studies in diagnosed cancer patients
Foci on imaging • NCI:Development and optimization of cancer specificCAD methods • NIBIB: Development of advanced algorithms and generic image processing methods, code documentation, open source software. • NLM: Open source software and related data processing platforms. • NSF: Advanced algorithm development, specialized hardware, GRID computing resources. • FDA: Development of standards for database development and • NIST:Measurement of performance of application specific software.
Imaging methods validated as cancer biomarkers. • Objectives: • Increase imaging studies, using standardized acquisition protocols, in NCI-funded therapy trials • Collate imaging data from all NCI-funded trials, e.g., in Cancer Centers, Cooperative Groups, CCR, etc. • Engage FDA through Inter Organization Task Force • Develop cadre of oncology imaging specialists in Cancer Centers • Develop functional imaging committees in all Cooperative Groups • Develop volumetric and functional “RECIST” criteria
CIP Near Term Goals: Data CollectionDevelop validated data collections: • Lung nodules (FNIH Demonstration Project) • for Detection, Classification, rx. Response • Liver mets - rx response • Colon polyps - screening detection, classification • Breast digital mammo - detection, classification
Clinical Imaging Concerns • Only 2% of all cancer patients are in formal clinical trials • Unless genetics is found to be deterministic, (all) cancer therapy will continue to be experimental • Conventional diagnostic imaging provides (barely quantitative) information when following a course of therapy