Download
1 / 29
290 likes | 637 Views
Long Term Conditions Risk Stratification Dr Junaid Bajwa Conway Medical Centre, Greenwich. About me. GP Principal, Greenwich RCGP Clinical Commissioning Champion Associate in Public Health, NHS Greenwich Medicine ’ s Management Lead NHS Greenwich GP Appraiser NHS SEL Chair Greenwich LMC

E N D
Long Term Conditions Risk Stratification Dr Junaid Bajwa Conway Medical Centre, Greenwich
About me GP Principal, Greenwich RCGP Clinical Commissioning Champion Associate in Public Health, NHS Greenwich Medicine’s Management Lead NHS Greenwich GP Appraiser NHS SEL Chair Greenwich LMC Education Lead GPCC Prepare to Lead alumni, NHS London
Multimorbidity: LTC • The majority of >65s have 2+conditions, & the majority of >75s have 3+ conditions • More people have 2 or more conditions than only have 1
Most people with any long term condition have multiple conditions in Scotland
The working lunch….. • 16 face to face 10 minute appts • Telephone encounters: 5-10 • Home visits (2-3) • Referrals: 3 (am) • Review blood tests/Investigations • Post/ Fax/ Email (75-100 letters per day) • 16 face to face 10 minute appts • Referrals: 3 (pm) What about: QoF/ LES/DES/ CIS/ Additional Services/ Child Protection/ GSF/ Information Governance/ CQC/ PRG/ Practice Meetings/ KPI’s/ Audit: Research/ Reviewing Prescribing/ HR issues/ LMC/ Public Health/ CCG ….(+++++++++++)…. Stepping outside the chaos to manage LTC holistically Proactive, not reactive medicine
GP’s and Nurses in deprived areas struggle with LTC’s “Demoralising” “Exhausting” “If you’re too caring ... you’ll crack up in a place like this. Our boundaries lie where they are because they have to at the moment” “I feel like a wrung-out rag at the end of consultations”
"Commodities are fungible, goods tangible, services intangible, and experiences are memorable." (Lee) Proactive management, not reactive Self Management • systematic transfer of some knowledge and power to maximise self-management and choice, where the GP acts as a navigator. Motivating Staff and Patients • Focus on compassion, autonomy, mastery and purpose • (correspondence (personalized, targets individualized), pt experience, face/face, telephone) • How can we do the right thing, but also make the lives of those around us easier at the same time
Opportunities & challenges? ‘A pessimist sees the difficulty in every opportunity, … an optimist sees the opportunity in every difficulty’ Sir Winston Churchill
Long Term Conditions Module Improving the experience of healthcare for those with long term conditions
Risk Stratification • The dilemma of "defining risk" for our patients on long-term conditions • Is it just the number of registers? • What about outside Qof: parkinsons, cirrhosis, inflammatory bowel disease….children…. • Existing: • Hospital Admission Risk programme (HARP)High–impact User Manager (HUM)Patient At Risk of Re-hospitalisation (PARR)Probability of repeat admissions (Pra) tool • http://www.yourdiseaserisk.wustl.edu/Looks at: Cancer/Diabetes/Heart Disease/Osteoporosis/Stroke • http://www.readmissionscore.org/Heart Attack/ Heart Failure/ Pneumonia
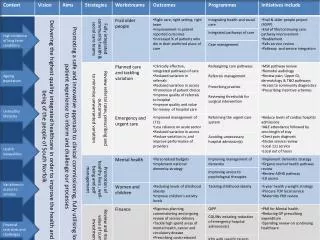
What if we used what we have? Metrics Long Term Conditions HbA1c Cholesterol BP MRC eGFR* BMI Waist circ Audit C score PHQ9 Being Housebound No of repeat Age >75 Being a smoker Cancer, COPD, Asthma, Diabetes, CKD 3,4,5, Hypertension, Rh Arthritis, AF, HF, Hypertension, Mental Health condition, LD, Dementia, Parkinsons, Cirrhosis, being on the GSF, Inflammatory Bowel Disease, Stroke/TIA, Osteoporosis
What if we used what we have? Metrics Long Term Conditions (Modifiable) (Fixed) HbA1c Cholesterol BP MRC eGFR* BMI Waist circ Audit C score PHQ9 Being Housebound No of repeat Being a smoker Cancer, COPD, Asthma, Diabetes, CKD 3,4,5, Hypertension, Rh Arthritis, AF, HF, Hypertension, Mental Health condition, LD, Dementia, Parkinsons, Cirrhosis, being on the GSF, Inflammatory Bowel Disease, Stroke/TIA, Osteoporosis Age >75
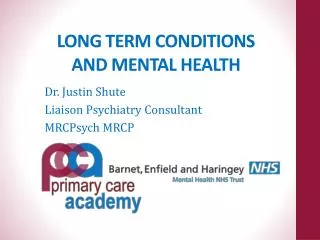
Within the metric….RAG Metrics RAG: R-2pts / A-1pt / G-0pt HbA1c Cholesterol BP MRC eGFR* BMI Waist circ Audit C score PHQ9 Being Housebound No of repeat Age >75 Being a smoker G (6.5-7.5), A (7.5-8.5); R (>8.5) > 4:2: A: 1 pt if above this ratio (>150/90; if DM/CKD/CHD >140/90) 1 pt if above G: 3,A: 4, R: 5 G (CKD2 60-89); A (CKD3 30-59); R (CKD4,5 ie < 29) A: (Obese**) R (:morbid obesity) A: 1 pt if above norm R: (>5) (last recorded within 3m) R: 15-27; A: 5-14 A: 1 point Repeat medications (>5): A 1 pt if above A 1 pt if above 75 A 1pts
Managing the chaos: Proactive vs Reactive Cumulative totals within each of the categories would then allow a 360° review of your registered population Could you then establish a set of rules re: appointments; removing the monthly letters for each review/ reduce waste in the system; offer extended appointments with a focus on self management- improving the patient experience
MSDi LTC Module The software will allocate a R,A,G, status to patients based on: The number of long term conditions they have Indicators used to define whether those conditions are optimally managed No of visits a patient has made to the surgery over the last 12 m Flexible: to allow for user defined thresholds and weightings to be allocated to each of the above parameters A care plan will be generated for the patient which will include the number of appointments that a patient will have over the following 12 m which are dedicated to the optimal management of that patients conditions. The software is practice based At locality level anonymised data can be aggregated and accessed through a web-based portal, allowing risk to be stratified across a geography.
PDSA: future add ons • PDSA cycle • Coding: Number of hospital admissions A(2); R(>3); • Quantify length of stay in hospital • QRISK®2 calculates your risk of cardiovascular disease(R >30%) (A>20) • QDScore® algorithm calculates your risk of Type 2 diabetes.) • QoL score (would be useful to include this metric- we do not currently assess this in primary care) • Looking at social determinants of health: e.g. personal/ household income, social housing, postcode, use of carers, social isolation “Not all that can be counted, counts. And not all that counts can be counted.” -- Albert Einstein
Improving the Patient Experience SDI. 12.GB.107042.SL Date of Preparation: May 2012
For More Information: • MSDinformatics Stand 171 in main hall • Call 01992 455 400 • Email: msdi@merck.com