Download
1 / 1
10 likes | 98 Views
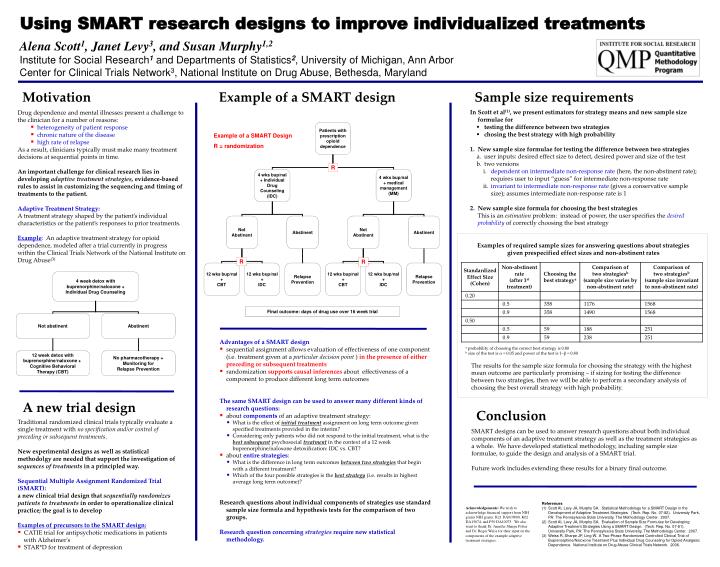
Using SMART research designs to improve individualized treatments. Alena Scott 1 , Janet Levy 3 , and Susan Murphy 1,2 Institute for Social Research 1 and Departments of Statistics 2 , University of Michigan, Ann Arbor

E N D
Using SMART research designs to improve individualized treatments Alena Scott1, Janet Levy3, and Susan Murphy1,2 Institute for Social Research1 and Departments of Statistics2, University of Michigan, Ann Arbor Center for Clinical Trials Network3, National Institute on Drug Abuse, Bethesda, Maryland Motivation Sample size requirements Example of a SMART design In Scott et al(1), we present estimators for strategy means and new sample size formulae for • testing the difference between two strategies • chosing the best strategy with high probability 1. New sample size formulae for testing the difference between two strategies • user inputs: desired effect size to detect, desired power and size of the test • two versions • dependent on intermediate non-response rate (here, the non-abstinent rate); requires user to input “guess” for intermediate non-response rate • invariant to intermediate non-response rate (gives a conservative sample size); assumes intermediate non-response rate is 1 2. New sample size formula for choosing the best strategies This is an estimation problem: instead of power, the user specifies the desired probability of correctly choosing the best strategy • Drug dependence and mental illnesses present a challenge to the clinician for a number of reasons: • heterogeneity of patient response • chronic nature of the disease • high rate of relapse • As a result, clinicians typically must make many treatment decisions at sequential points in time. • An important challenge for clinical research lies in developing adaptive treatment strategies, evidence-based rules to assist in customizing the sequencing and timing of treatments to the patient. • Adaptive Treatment Strategy: • A treatment strategy shaped by the patient’s individual characteristics or the patient’s responses to prior treatments. • Example: An adaptive treatment strategy for opioid dependence, modeled after a trial currently in progress within the Clinical Trials Network of the National Institute on Drug Abuse(3) Examples of required sample sizes for answering questions about strategies given prespecified effect sizes and non-abstinent rates Final outcome: days of drug use over 16 week trial • Advantages of a SMART design • sequential assignment allows evaluation of effectiveness of one component (i.e. treatment given at a particular decision point ) in the presence of either preceding or subsequent treatments • randomization supports causal inferences about effectiveness of a component to produce different long term outcomes The same SMART design can be used to answer many different kinds of research questions: • about components of an adaptive treatment strategy: • What is the effect of initial treatment assignment on long term outcome given specified treatments provided in the interim? • Considering only patients who did not respond to the initial treatment, what is the best subsequent psychosocial treatment in the context of a 12 week buprenorphine/naloxone detoxification: IDC vs. CBT? • about entire strategies: • What is the difference in long term outcomes between two strategies that begin with a different treatment? • Which of the four possible strategies is the best strategy (i.e. results in highest average long term outcome)? Research questions about individual components of strategies use standard sample size formula and hypothesis tests for the comparison of two groups. Research question concerning strategies require new statistical methodology. a probability of choosing the correct best strategy is 0.80 b size of the test is α = 0.05 and power of the test is 1−β = 0.80 The results for the sample size formula for choosing the strategy with the highest mean outcome are particularly promising – if sizing for testing the difference between two strategies, then we will be able to perform a secondary analysis of choosing the best overall strategy with high probability. A new trial design Conclusion • Traditional randomized clinical trials typically evaluate a single treatment with no specification and/or control of preceding or subsequent treatments. • New experimental designs as well as statistical methodolgy are needed that support the investigation of sequences of treatments in a principled way. • Sequential Multiple Assignment Randomized Trial (SMART): a new clinical trial design that sequentially randomizes patients to treatments in order to operationalize clinical practice; the goal is to develop • Examples of precursors to the SMART design: • CATIE trial for antipsychotic medications in patients with Alzheimer's • STAR*D for treatment of depression SMART designs can be used to answer research questions about both individual components of an adaptive treatment strategy as well as the treatment strategies as a whole. We have developed statistical methodology, including sample size formulae, to guide the design and analysis of a SMART trial. Future work includes extending these results for a binary final outcome. • References • Scott AI, Levy JA, Murphy SA. Statistical Methodology for a SMART Design in the Development of Adaptive Treatment Strategies. (Tech. Rep. No. 07-82). University Park, PA: The Pennsylvania State University, The Methodology Center. 2007. • Scott AI, Levy JA, Murphy SA. Evaluation of Sample Size Formulae for Developing Adaptive Treatment Strategies Using a SMART Design. (Tech. Rep. No. 07-81). University Park, PA: The Pennsylvania State University, The Methodology Center. 2007. • Weiss R, Sharpe JP, Ling W. A Two-Phase Randomized Controlled Clinical Trial of Buprenorphine/Naloxone Treatment Plus Individual Drug Counseling for Opioid Analgesic Dependence. National Institute on Drug Abuse Clinical Trials Network. 2006. Acknowledgements: We wish to acknowledge financial support from NIH grants NIH grants: R21 DA019800, K02 DA15674, and P50 DA10075. We also want to thank Dr. Jennifer Sharpe Potter and Dr. Roger Weiss for their input on the components of the example adaptive treatment strategies.