Download
1 / 42
420 likes | 435 Views
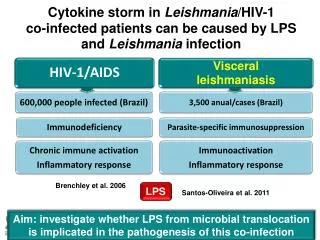
Explore the comprehensive approach of Brazil's response to HIV/AIDS, including funding, decentralization, and human rights perspective. Learn about key milestones, current trends, and future priorities in the country's battle against the epidemic.

E N D
The National Response to HIV/AIDS in Brazil Brazilian STD/AIDS Program Ministry of Health
Country Profile • Population (2005) – 185 mln • Federative Republic with 27 States • Municipalities - 5,561 • Territory: 8,5 mln sq km • GNP (2004) US$ 750 bi • Per capita GNP (2004) - US$ 4,041 • HDI Rank (2005) - 63th (0.792)
Epidemiological Profile • Accumulated AIDS cases (06/2005): 371,827 • AIDS incidence rate (2004): 17,2/100,000 inhabitants • Estimated n. of PLWHA (2004): around 600,000 • Prevalence: (15 to 49 years of age) • 2000: 0.61% • 2004: 0.61% • Aids deaths (1980-2004): 171,923 • Mortality rate: 6,1/100,000 (2004) inhabitants
Current epidemiological trends • Relative stabilization, -decreasing: southeast, MSM, IDU -Stabilized: big cities • Increasingly affecting: - Heterosexuals - Women - Low-income groups - Smaller cities
Total investment in STD/AIDS control program by the Federal Government. Brazil, 1997-2005 World Bank Loan 11% 1997 to date: US$ 3.5 billion (HIV response) US$ 2 billion for ART Average investment per year: US$ 400 MILLION National budget Source: PN STD-AIDS//MOH 89%
The “backbone” of the Brazilian Response: the Public Health System The 1988 Brazilian Constitution: access to health is a basic right • Main precepts: - comprehensive approach - universal access and equity - civil society participation • Key feature: decentralization • Virtuous circle (AIDS Programmes Public Health System)
History of Health Policy • Actions on health promotion and disease prevention were a responsibility of the Social Security Institute • 1988 – Federal Constitution – Health as Right of all and a duty of the State. • 1990 - Law 8.080 – Creation of the Unified Health System.
History of Health Policy • Regulations of the Unified Health System: • 93 fund to fund transfer of Health financial resources. • 96 increase of funds transfers. • Assistance regulations: • organization of the System through regional assistance policies. • introduction of criteria for the inclusion of states and municipalities into the System and strengthening of decentralization.
Political Response to the epidemic* • 1982-1985 • Notification of the first AIDS cases; creation of the State of São Paulo Aids Program; establishment of the first NGOs; negligence of governmental authorities; panic and prejudice • 1986-1990 • Creation of a response at national level; pragmatic approach about the epidemic; spread of NGOs all over the country; mobilization de People Living with HIV/Aids • 1990-1992 • Interruption of some of the key elements of the National Program; opposition between the NAP and the organized civil society; Deterioration on international relations *(Parker, 1997)
1992-1997 Return to the dialog with NGOs; First Agreement with the World Bank (AIDS I); Adoption of a policy of universal access to ARV drugs 1998-2006Decentralization/Disconcentration; Empowerment of the social movement; Consolidation of public policies; Enlargement of partnerships; Human Rights as a transversal issue; AIDS II and AIDS III; Horizontal Technical Cooperation; Consolidation of the process of cooperation with international agencies; Visibility and recognition at international level
Priorities for 2006-2007 • Universal access to Prevention, Care and Treatment • Strengthen, implementation and extend of the prevention, promotion and care policies related to HIV and Aids on the scope of the Health system network (SUS), with a comprehensive approach and according to the SUS principles. • Promote the defense of human rights and reduce stigma and discrimination of people living with HIV and aids and of the most vulnerable population.
Major features of theBrazilian Response Country-driven approach: • Social Control: robust participation by civil society in decision making and implementation • Balanced prevention and treatment approach • Comprehensive ethical and rights-based approach • Early response by government (since 1983) • Multi-sectoral mobilization Human Rights perspective in all the strategies and actions
National Health System (SUS) Principles Ministry Of Heath Unified Decentralized Participation of civil society in decision making National Health Council State Health Secretaries State Health Councils Municipal Health Secretaries Municipal Health Councils
Aids National Management Ministry Of Heath 3 Ones in practice Health Surveillance Secretariat National STD/AIDS Program National HIV/AIDS Commitee UNAIDS Thematic Group AIDS Business Council
MINISTRY OF HEALTH SECRETARIAT FOR HEALTH SURVEILLANCE UNAIDS THEMATIC GROUP NATIONAL AIDS COMMISSION GTZ NATIONAL STD AIDS PROGRAM CDC ADMINISTRATIONS’ COMMITTEE COM. FOR INTERACTION WITH CIVIL SOCIETY MOVEMENTS International Center for Technical Cooperation - ICTC PRIVATE SECTOR’S NATIONAL COUNCIL FOR HIV / AIDS ADVISORY COMMITTEES* INTERNATIONAL COOPERATION ADVISORY COMMUNICATION ADVISORY INFORMATION SYSTEMS’ ADVISORY PLANNING ADVISORY Civil Soc. And H. R. Assist. and treat. Lab. Surv. M&A Hum Res. Res. Tech Dev. Adm. Prevention STD * Advisory Committees STRUCTURE OF THE NAP
Prevention Framework • Expand access to prevention commodities (male/female condoms, lubricating gel, harm reduction supplies) • Extend joint activities with CSO’s, CBO’s, uniformed services, social movements and other government programs • Increase coverage in poorest areas, emphasizing counselling and testing through the primary health system • Implement education programs throughout the public school system at all levels - Prevention Program in Public Schools in Brazil-2005
Prevention Program in Public Schools in Brazil-2005 • Number of questionnaires analyzed: 161.679 • % of brazilian schools = 78% • # of schools with STI/Aids as part of school program = 97.600 • % of schools with STI/Aids as part of school program =60,4% • # of schools distributing condoms = 9.200 • % of schools distributing condoms = 9,1% (17% in high school) • % of schools work with topic: sexual and reproductive health as part of the school program = 45,3% • % of schools work with topic: adolescent pregnancy as part of the school program = 51,8% • % of schools work with topic: drugs as part of the school program = 71%
Regular condom use (last 12 mo.) among those aged 16-65 (2005) 40% 35,4% 35% 30% 23,9% 25% 20% 15% 10% 5% 0% 1998 2005 Fonte: Pesquisa CEBRAP, 2005.
Percentage change in condom use among young people in first sexual intercourse (1) 1986 (2) 1998 (3) 2003 0 10 20 30 40 50 60 70 Sources: (1) BEMFAM (2) CEBRAP/MH/PN-STD/AIDS/SVS (3) MH/PN-STD/AIDS/SVS – (PCAP_BR_2003,IBOPE)
Harm Reduction: a basic prevention strategy • Estimated number of IDUs in Brazil: 193,000 (Source: PCAP, 2004) • Percentage of IDUs who reported no syringe/needle sharing: 76% (Source: PCAP - 2004) • AIDS cases among IDUs: • 1993 = 4926 cases (28.0% of total reported cases) • 2003 = 1871 cases (10.2% of total reported cases)
Treatment, Care and Support • 1980’s: • Treatment and care centered around OI treatment • Capacity and institution building, training • 1988: AZT is introduced in the Brazilian market • 1991: distribution of AZT through the public health system is initiated • 1996: “Sarney” Law 9313 (Universal access to HAART) • 1997-1998: establishment of monitoring and logistic systems
People living with AIDS under ARV treatment. BRASIL, 1997 A 2006 Fonte: PN DST/Aids, MS
Average cost of ARV therapy per patient/year (US$). Brazil, 2005 7000 6240 6000 5486 Introduction of expensive new ARVs 5000 4603 4000 • Substantial falls in prices of second-line patented drugs have ceased • Number of people using them has increased dramatically 3464 3000 Thousands (US$) 2500 2210 2000 1500 1359 1336 1000 0 1997 1998 1999 2000 2001 2002 2003 2004 2005* Year
Antiretroviral drugs distributed through the Brazilian public health system (and year of introduction) ITRN and ITRNt IP • ZIDOVUDINE (1993)* • ESTAVUDINE (1997)* • DIDANOSINE (1998)* • LAMIVUDINE (1999)* • ABACAVIR (2001) DIDANOSINE EC (2005) TENOFOVIR (2003) • RITONAVIR (1996)* • SAQUINAVIR (1996)* • INDINAVIR (1997)* • NELFINAVIR (1998) • AMPRENAVIR (2001) • LOPINAVIR/r (2002) • ATAZANAVIR (2004) ITRNN FUSION INHIBITOR • NEVIRAPINE (2001)* • EFAVIRENZ (1999) • ENFUVIRTIDE (2005) *Brazilian local production
0.90 0.81 0.80 0.70 0.60 0.56 0.50 0.43 0.40 0.38 0.30 0.28 0.26 0.26 0.24 0.20 0.10 0.00 1997 1998 1999 2000 2001 2002 2003 2004 Average of AIDS related hospitalizations per patient / year Average number of AIDS-related hospitalizations per patient / year
250,000 200,000 150,000 100,000 50,000 0 1997 1998 1999 2000 2001 2002 2003 2004 Hospitalizations recorded in the Public Health System Estimated number of hospitalizations that would have been registered, assuming 1996 average * “potential” figure is based on the 1996 average of AIDS-related hospitalizations Difference between the number of AIDS-related hospitalizations effectively registered and its potential*
Total number and estimated value of hospitalizations averted (non-cumulative figures) $600,000,000.00 180,000 Total: Hospitalizations avoided: 791,069 Total savings: US$ $2,289,654,584 160,000 $500,000,000.00 140,000 $400,000,000.00 120,000 Expenditures (in US$) Number of hospitalizations 100,000 $300,000,000.00 80,000 $200,000,000.00 60,000 40,000 $100,000,000.00 20,000 $0.00 0 1997 1998 1999 2000 2001 2002 2003 2004 Estimated value of hospitalizations avoided Estimated number of hospitalizations avoided
Monitoring and Evaluation Framework • 2003-2005: design of an updated, integrated and comprehensive national M&E plan • Current phase: • implementation of the national M&E plan and its real-time informational system(www.aids.gov.br/monitoraids); • Capacity Building in M&E (health professionals, public health managers, universities, NGOs etc) • Implementation of five sites of excellence in M&E
South-South Cooperation: Network for Technological Cooperation in HIV/AIDS Launched in 2004, involving Argentina, Brazil, China, Cuba, Nigeria, Russia, Thailand and Ukraine Key support provided by the Ford Foundation: US$ 1 million Objectives: technology transfer, R&D and production: - antiretrovirals - vaccines and microbycides - condoms - laboratory supplies
The GCTH – Group for Horizontal Technical Cooperation. Launched in 1995 to establish direct cooperation between the Latin American and Caribbean State Governments on HIV and AIDS control and prevention. Objectives: - Reference for building up regional statements for International Events. - Courses , Conferences and Forums. - Development of the Price Bank. - Development of web-page and improvement of electronic communication.
Other South-South Cooperation Initiatives Technical Areas: Institutional development, management and capacity building Care and support Clinical management Antiretroviral logistics and management Epidemiological surveillance Promotion of safer sexual practices Promotion of human rights Advocacy and Civil Society participation Care and support for HIV+ pregnant women and children exposed to HIV
International Cooperation with Developed Countries Institutions involved: ANRS (France), CDC, USAID, Ford, GTZ, DFID United Nations :UNAIDS, UNFPA, UNICEF, UNODC, UNESCO, ILO, Thematic areas: Monitoring and Evaluation; Promotion of safer sexual practices Promotion of human rights Advocacy andCivil Society participation Scientific and technological development
Based on “Horizontal” Technical Cooperation • sharing experiences - not “vertical” building partnerships commitment to attend to specific needs of each country – “tailored” approach donor X recipient??role of multilateral partners?
Laços Sul Sul – Lazos Sur-Sur 8 countries - Brazil, Cabo Verde, Guine-Bissau, São Tome e Principe, Bolivia, Nicaragua e Paraguai, Timor Leste based initially on bilateral projects with Brazil – technical cooperation and provision of ARV partnership with Unicef (and Unaids) – since 2004
Laços Sul Sul - main aspects so far a truly horizontal type of cooperation – every country has some experience to share based entirely on the 3 Ones Principles countries ownership – part of the national plans some concrete results – increased access to prevention and treatment services for women and children Unicef acts as a “focal point” in-country – within UN HIV/AIDS Team Groups
Main challenges each country at its own pace – partnership may help “speed up” some national responses to AIDS fragile health systems / governance – LSS Initiative may help countries with difficulties to scale up access to prevention and health services provision
International Center for Technical Cooperation: a Joint Brazil/UNAIDS Initiative • Created in 2005, the ICTC aims to create and strengthen national technical capabilities forimplementing comprehensive AIDS responses through horizontal technical cooperation; • Example of activities undertaken: • Coordination of technical missions in Honduras, Nicaragua, Peru, Ecuador and Bolivia • Identification of technical assistance needs of Latin American countries receiving financial support from the Global Fund • Total investments: • Brazilian Government (US$ 500,000), UNAIDS (US$ 500,000), DFID (£ 250,000 - under negotiation), GTZ (€ 250,000 – under negotiation)

![OVERVIEW OF THE HIV/AIDS SITUATION IN GHANA AND GHANA’S NATIONAL RESPONSE (GHANA MULTI-COUNTRY HIV/AIDS PROGRAM [MAP] PR](https://cdn0.slideserve.com/353831/slide1-dt.jpg)