Download
1 / 13
150 likes | 383 Views
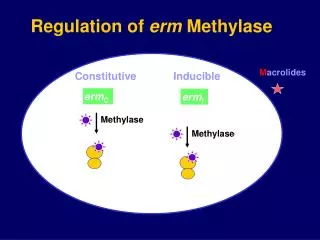
M acrolides. Methylase. Methylase. Methylase. Regulation of erm Methylase. Constitutive. Inducible. erm C. erm I. C. C. Inducible Macrolide-Lincosamide-Streptogramin B (MLS B ) Phenotype. Zone of Inhibition. E. E. Blunted Zone. Clinical Implications.

E N D
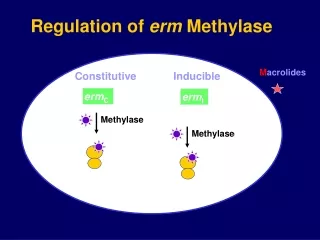
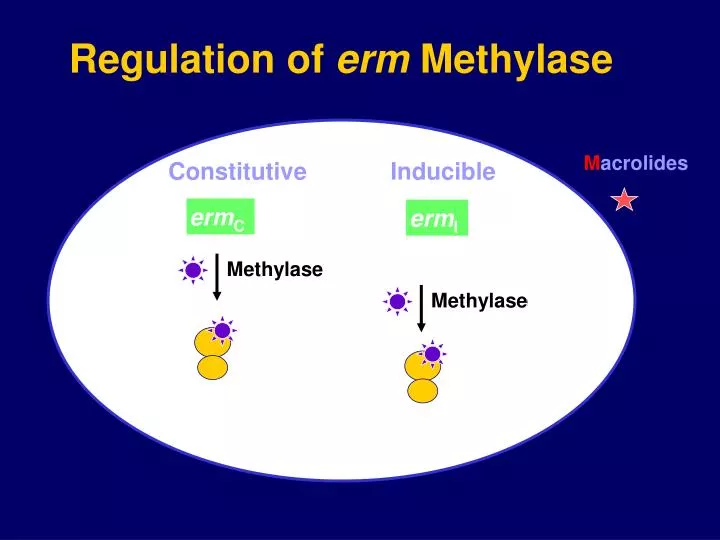
Macrolides Methylase Methylase Methylase Regulation of erm Methylase Constitutive Inducible ermC ermI
C C Inducible Macrolide-Lincosamide-Streptogramin B (MLSB) Phenotype Zone of Inhibition E E Blunted Zone
Clinical Implications Constitutive mutants, which can occur at a frequency of ~10-7cfu, may be selected during a course of clindamycin therapy in patients with infections due to inducible clindamycin-resistant strains of S. aureus
Genome and Virulence of CA-MRSA • CA-MRSA isolate from one fatal case sent to Japan (PFGE subtype MR 14A) • CA-MRSA (MW2) genome sequenced • MW2 grows faster than HA-MRSA strains • MW2 has SCCmec type IVa (types I-III typically seen in HA-MRSA strains) • MW2 has unique virulence genes (including PVL) • Lethal dose of MW2 in an animal model is five times less than a comparison Japanese HA-MRSA strain Baba et al. Lancet. 2002; 359:1819-27
Panton-Valentine Leukocidin (PVL) • S. aureus cytotoxin formed from 2 synergistic proteins • Causes tissue necrosis (skin and mucosa) and leukocyte destruction by forming pores in cellular membranes • PVL identified in 7 isolates from fatal CA-MRSA MN patients; 6 with necrotizing pneumonia
Effects of PVL on PMNs Without PVL With PVL
Exotoxin Genes and Gene Alleles • 26 CA-MRSA and 26 HA-MRSA isolates underwent polymerase chain reaction to detect gene sequences • Panton-Valentine leukocidin*, staphylococcal enterotoxins A,C, H, and K, accessory gene regulator 3 and SCCmec IV were significantly more likely to be found among CA-MRSA isolates • Staphylococcal enterotoxins D, G, I, J, M, N, O, accessory gene regulator 2, and SCCmec II were significantly more likely to be found among HA-MRSA isolates * Produces exotoxin causing tissue necrosis and leukocyte destruction, has been associated with cases of necrotizing pneumonia, skin abscesses
Management of Skin and Soft Tissue CA-MRSA Abscesses Observational study: 69 children, TX 5/02-3/03, ER/acute care clinic • Incision and drainage effective management (only 7% given initial antibiotic active against their isolate) • Predictor of hospitalization was initial lesion > 5 cm (p=0.004) Lee. Ped Infec Dis J. 2004; 23: 123-7.
Hospital Transmission of CA-MRSA • 8 postpartum women developed skin and soft tissue infections • 5 re-hospitalizations, 3 required surgical drainage • Isolates indistinguishable by PFGE • CA-MRSA strain (MW2) Saiman. Clin Infect Dis. 2003; 37:1313-9.
Conclusions • CA-MRSA strains have distinct molecular and microbiologic features compared with HA-MRSA strains • The emergence of MRSA in the general population has important clinical implications because empiric therapy is generally a beta-lactam antimicrobial agent • Additional evaluation needed on treatment options for non-severe infection • CA-MRSA susceptibility trends in other antimicrobial classes should be monitored
Conclusions (cont.) • More information is needed on the clinical impact of inducible clindamycin-resistant strains • More information is needed on the impact of bacterial virulence factors on severity of CA-MRSA infections • Risk factor studies are needed to identify persons at risk and optimal methods of prevention • CA-MRSA strains have been detected in hospital settings and have been associated with nosocomial infection
Antimicrobial Resistance “… the microbes are educated to resist penicillin and a host of penicillin-fast organisms is bred out which can be passed on to other individuals and perhaps from there to others until they reach someone who gets a septicemia or a pneumonia which penicillin cannot save. In such cases the thoughtless person playing with penicillin treatment is morally responsible for the death of the man who finally succumbs to infection with the penicillin-resistant organism. I hope this evil can be averted.” ~ Sir Alexander Fleming, New York Times, 6/26/45
Acknowledgements MDH: Joanne Bartkus, John Besser, Dave Boxrud, Jessica Buck, Elizabeth Cebelinski, Kathy Como-Sabetti, Richard Danila, Anita Glennen, Billie Juni, Kathy LeDell, Beth Shade, Sarah Vetter Active Bacterial Core Surveillance Staff, Infection Control Practitioners and Microbiologists in CT, GA, MD, MN; Monica Farley, Lee Harrison CDC: Scott Fridkin, Jeff Hageman, Monina Klemens, Melissa Morrison and Fred Tenover