Download
1 / 60
600 likes | 717 Views
The Endocrine System. Electrochemical Signals. Influences metabolic activities by means of hormones Chemical messengers released into the bloodstream to be transported throughout the body. Lag time in response Nervous = (near) immediate Endocrine = seconds to days

E N D
Electrochemical Signals • Influences metabolic activities by means of hormones • Chemical messengers released into the bloodstream to be transported throughout the body. • Lag time in response • Nervous = (near) immediate • Endocrine = seconds to days • Once initiated, hormonal responses tend to be more prolonged than nervous responses • Study of hormones & endocrine organs = endocrinology
Processes controlled by Hormones • Reproduction • Growth & development • Mobilizing body’s defense against stressors • Maintaining electrolyte balance • Maintaining nutrient balance • Regulating cellular metabolism • Maintaining an available energy source
Overview • Endocrine glands, compared to other systems: • Called glands – main purpose: secrete • Small glands, less than 2lbs worth • Widely scattered throughout the body – usually near their target organs • Endocrine vs. exocrine • Exocrine – have ducts • Non hormonal products are routed to a membrane surface • Endocrine – ductless • Release hormones into surrounding tissue of organs that are richly vascular • Easy to be released into bloodstream of the appropriate organ. • Most are physically arranged into branching networks to maximize the spread of hormones
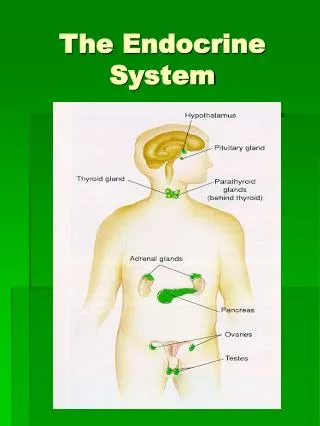
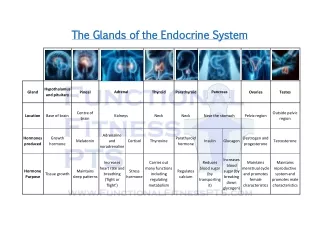
Endocrine Glands • Pituitary • Thyroid • Parathyroid • Adrenal • Pineal • Thymus • Organs that contain endocrine tissue & produce hormones • Pancreas • Gonads (testes & ovaries) • Neuroendocrine organ = hypothalamus
Chemistry of Hormones • Hormones are chemical substances, secreted by cells into extracellular fluids, that regulate the metabolic function of other cells in the body. • 2 classes: amino-acid based vs. steroid • Most hormones are amino-acid based • Simple derivates: amines, thyroxine, peptides • Steroid hormones are synthesized from cholesterol • Gonadal & adrenocortical hormones • “3rd” class: eicosanoids • Leukotrienes & prostaglandins • Local hormones: very specific functions • Leukotrienes: mediate inflammation & slow allergic reactions • Prostaglandins: raising BP, increases birth contractions of the uterus
Mechanisms of Hormone Action • Hormones act on target cells by altering cell activity. • Increase or decrease rates of normal cellular activity • Precise response depends on the target cell • Hormonal stimulus should produce one of the following changes • Alters permeability of the plasma membrane by opening/closing ion channels • Stimulates synthesis of proteins or regulatory molecules (like enzymes) within the cell • Activiates/deactivites enzymes • Induces secretory activity • Stimulates mitosis
Hormone – Target Cell Specificity • Each hormone only can only work on certain tissues • Specific protein receptors on a cell membrane will only receive the chemical message from certain hormones • EX) Adrenocorticotrophic hormone (ACTH) receptors are only found on the adrenal cortex, where as thyroxine receptors are found on nearly all cells of the body. • 3 important factors to ensure proper target cell activiation • Consistent blood levels of hormone • Relative number of receptors for that hormone on/in the target cells • The affinity (strength) of the bond between the hormone and the receptor
Hormone Receptors • Receptors are dynamic structures • Will change in response to need • In response to rising blood levels of hormone, more receptors will be created – up-regulation • Prolonged exposure to high levels of a hormone could cause desensitization of receptors, so receptors will respond less vigorously to hormones – down-regulation • Hormones don’t always affect their own targets, but how they respond to other receptors • EX) Progesterone reduces estrogen receptors in the uterus • Estrogen causes the same cells to produce more progesterone receptors – enhancing the ability to respond to progesterone.
Half-Life, Onset & Duration of Hormone Activity • Hormones are potent • Profound effects in very low concentrations • Concentration of a circulating hormone at any time reflects • Its rate of release • Speed of its inactivation and removal from the body • Some hormones are rapidly degraded by enzymes • Most are removed from the blood by the kidney/liver enzymes • Breakdown products of hormones released mostly in urine (rarely in feces) • How long a hormone stays in the blood is its half-life • Ranges from fraction of seconds – 30 minutes • Most hormones effects are seen immediately, but steroid hormones require hours, sometimes days before their effects are seen. • Some hormones, like testosterone, are secreted in an inactive form, and must be activated, when ready, by the target organ • Duration of hormone in bloodstream ranges from 20 minutes – hours • Hormone levels are precisely controlled to maintain consistent levels while the body is continuously changing
Control of hormone release • Negative feedback • As hormone levels rise, they activate the target cells • Once the desire effect is achieved, hormone production will be inhibited further. • As a result, hormone blood levels vary only within a narrow “desirable” range.
Hormonal Stimuli • Stimuli: Humoral, Hormonal, or Neural • Humoral: hormones released in response to nutrition/ionic needs • Ex) The parathyroid detects low blood calcium, initiates the secretion of PTH (which stimulates the uptake of calcium from bones), thus raising blood calcium • Once blood calcium levels have stabilized, the production of PTH ceases • Other examples include the body’s use of insulin (sugars) & aldosterone (maintains sodium balance)
Neural & Hormonal Stimuli • Neural: nerve fibers stimulate the release of hormones • Sympathetic nervous system • Adrenal medulla releases epinephrine during periods of stress • Hormonal: Many endocrine glands release their hormones in response to other hormones • The hypothalamus-pituitary relationship is the core of the study of endocrinology • Hypothalamus release hormones to regulate and inhibit the pituitary, in turn… • The function of most anterior pituitary hormones is to initiate the release of other endocrine hormones (targeted organs) • Once those target hormones have been triggered, they will inhibit the production of more pituitary hormones
Neural Modulation • “On” and “off” factors • Hormonal, humoral & neural stimuli initiate the production of hormones • Negative feedback inhibit the overproduction of hormones • The nervous system can “override” the fairly strict functioning of the nervous system • Ex) During periods of stress, blood sugar levels rise because the hypothalamus and sympathetic nervous system are strongly activated • This ensures the body has enough fuel for more vigorous activity • The endocrine system would usually response to the increased sugar by?
Major Endocrine Organs: Pituitary Gland • Nestled in the sellaturcica of the sphenoid bone • About the size and shape of a pea on a stalk • The stalk, that connects to the hypothalamus is called the infundibulum(funnel shaped) • Two lobes: • Posterior Lobe - neurohypophysis • Neural tissue – nerve fibers & glia-like supporting cells • Releases neurohormones it receives from the hypothalamus • Not a true endocrine gland – just stores hormones from hypothalamus • Anterior Lobe - adenohypophysis • Completely glandular tissue • Releases numerous hormones
Pituitary Hypothalamic Relationship • Posterior lobe of the pituitary is actually part of the brain. • Downgrowth of hypothalamic (neural) tissue runs through the infundibulum • Two hormones are synthesized here: • Oxytocin & ADH (antidiuretic hormone) • All hypothalamic regulatory hormones are amino-acid based.
Structural/Functional relationships of the pituitary and the hypothalamus
Anterior Pituitary Hormones • Usually called the “master gland” • Produces many hormones, including most hormones that regulate other hormones • 6 distinct adenophyophyseal hormones • Creates POMC – pro-opiomelanocortin • A pro-hormone • Building block hormone – used to create many different molecules • Natural opiates – like endorphins • Melanocytes – break down melanin • 4 out of 6 of the distinct hormones are trophichormones • Regulate the secretion of other endocrine glands • TSH, ACTH, FSH, & LH
Growth Hormone • Anabolic steroid hormone • Stimulates most body cells to increase in size and divide • Major targets are bones and skeletal muscles • Stimulation along the epiphyseal plate leads to long bone growth • Promotes the creation of muscle mass in skeletal muscles • GH promotes protein synthesis • Encourages the use of fats for fuel, thus conserving glucose • Stimulates the uptake of amino acids from the blood and their incorporation into cellular proteins throughout the body • Stimulates the uptake of sulfur (needed to synthesize chondrotin sulfate) – helps form cartilage
Growth Hormone • Works via negative feedback, like all hormones • Secondary stimulation • Stress, nutritional factors, and sleep patterns • Highest levels during evening sleep • Highest total amounts during adolescene and then declines with age. • Secondary inhibition • Hyperlipidemia, hyperglycemia, obesity, emotional deprivation • Hyposecretion: • Pituitary dwarfism in children • Hypersecretion • Gigantism in children; acromegaly in adults
TSH: Thyroid Stimulating Hormone • TSH – thyrotropin • Stimulated by TRH (thyrotropin-releasing hormone) – a hypothalamic peptide • Pregnancy & cold temperatures can indirectly increase the production of TSH • Stimulates normal development and secretory activity of the thyroid gland • Rising blood levels of thyroid hormones will inhibit the further production of TSH • The hypothalamus will release somatostatin which will further inhibit the production of TSH • Hypersecretion: cretinism in children, myxedema in adults • Causes low thyroxine • Hyposecretion: Graves’ disease • Causes high thyroxine
ACTH: Adrenocorticotropic Hormone • Stimulates adrenal cortex to release corticosteroid s • This, in turn, releases glucocorticoids • Most importantly – helps the body resist stressors • ACTH release has a daily rhythm – peaks in early morning • Triggers for increase beyond normal limits include: • Fever • Hypoglycemia • Stressors of all types • Inhibited by the release of glucocorticoids • Hyposecretion: rare & idiopathic • Hypersecretion: Cushing’s disease
Gonadotropins • Follicle-stimulating hormone (FSH) & LH • Present in both males & females! • Regulate the functions of gonads • FSH stimulates gamete production • LH promotes production of gonadal hormones • In females, LH works with FSH to cause maturation of a follicle (immature egg) = ovulation • Promotes the synthesis of estrogen & progesterone • In males, LH stimulates interstitial cells to produce testosterone • LH is called ICSH in makes – interstitial cell-stimulating hormone
Gonadotropins • Absent in the blood of prepubertal boys & girls • When puberty starts, the anterior pituitary produces gondaotrope cells (building block of gonadotropins) – causing the gonads to mature • The hypothalamus produces GnRH – which promotes the production of FSH & LH • The gonadal hormones (estrogen, progesterone, & testosterone) suppress/inhibit the further production of FSH & LH • Hyposecretion: Failure to sexually mature • Hypersecretion: No important effects
Prolactin • PRL – protein hormone/similar to growth hormone • Produces by lactotropes – stimulates the gonads of some mammals • Well-documented – production of breastmilk • Evidence that PRL enhances testosterone production • PRH released by hypothalamus to stimulate prolactin production • PIH (Prolactin-inhibiting hormone) IS dopamine – prevents prolactin secretion • In males, PIH predominates, but in women, prolactin levels rise and fall with estrogen levels • Low estrogen stimulates PIH release & high estrogen promotes more prolactin production
Prolactin • Brief rise in prolactin levels accounts for breast tenderness & swelling just before menstruation • Since the PRL production is so brief, no milk is produced • In pregnancy, prolactin rises dramatically in the last trimester and milk production begins • Fun fact: prolactin levels can remain high as much as two years after breastfeeding ceases. • Hyposecretion: poor milk production in nursing women • Hypersecretion: Galactorrhea, cessation of mense in females, impotence and gynecomastia in males
Posterior Pituitary Hormones • Comprised largely of axons of hypothalamic neurons • Stores oxytocin & antidiuretic hormone (ADH) • These hormones are left “on demand”, when stimulated by nerve impulses from the hypothalamus • ADH & oxytocin are protein based hormones • Almost identical molecularly • VERY different functionally • ADH influences water balance • Oxytocin stimulates the contraction of smooth muscle
Oxytocin • Released in significantly high amounts during childbirth & nursing women • Oxytocin receptors peak near the end of pregnancy. • Stretching of the uterus and cervix as birth approaches sends sensory impulses directly to the hypothalamus • Hypothalamus makes more oxytocin and raises the blood level of oxytocin • Higher blood levels of oxytocin – expulsive contractions of labor gain momentum & end with labor • Oxytocin triggers milk ejection (“let down”) in women whose breasts actively produce milk in response to prolactin • Positive feedback – as demand for milk increases, MORE oxytocin is released, instead of being inhibited
Oxytocin • Synthetic oxytocin – Pitocin – can be used to artificially progress labor • Less frequently, oxytocics given to stop uterine/vaginal bleeding post-delivery • In non-lactating females, the non-pregnant & males: • Potent peptide plays a role in sexual arousal, when the body is primed for reproduction • Responsible in satisfaction in the sexual interaction • Overall, it is now readily known as the “attachment” hormone.
Antidiuretic Hormone (Vasopressin) • Diuresis: urine production • ADH: Inhibits or prevents urine formation • Prevents wide swings in water balance • Helps to avoid water overload or water dehydration • Hypothalamic neurons called osmoreceptors continually monitor solute & water concentration of the blood • When solutes make blood too concentrated • Ex) excessive perspiration, inadequate liquid intake, repeated vomitting • Osmoreceptors transmit excitatory impulses to the hypothalamic neurons to release ADH • This will tell the kidneys to reabsorb water into the bloodstream and produce less urine • When solute concentration declines, osmoreceptors are depolarized, stopping ADH production • ADH can also be triggered by pain, low blood pressure, and certain drugs: nicotine, morphine and barbiturates (mild sedation to anesthesia)
ADH - Vasopression • Hyposecretion: Diabetes insipidus • Characterized by excessive thirst and excretion of large amounts of severely diluted urine, with reduction of fluid intake having no effect on the concentration of the urine. • Drinking alcohol inhibits ADH = copious urine output • “hangover” – dehydrating effect of alcohol consumption from suppression of ADH production • Diuretic drugs antagonize the effects of ADH and cause water to be flushed from the body • Used to manage hypertension, edema (retention of fluids in tissues), typical in congestive heart failure • In high concentrations – ADH causes vasoconstriction – raising BP • Helpful in situations like severe blood loss
Thyroid Gland • Butterfly shape gland in the anterior neck, just inferior to the larynx, on the trachea • Two lobes – connected by isthmus (piece of tissue) • Internally: • Composed of hollow, spherical follicles • Cuboidal & squamous cells – produce thyroglobulin • Central cavity produces colloid, amber sticky material that stores iodine • Parafollicular cells: produce calcitonin
TH – thyroid hormone • TH – major metabolic hormone – iodine containing hormones: 2 types: • T4: thyroxine • Secreted by thyroid follicle • T3: triiodothyronine: • Converted by target organs from T4 • TH effects EVERYTHING except • The brain • Spleen • Testes • Uterus • Thyroid itself • In every cell of the body, T4 & T3 – stimulates glucose oxidation • Thus, increasing basal metabolic rate& body’s heat production
Transport & Regulation of T4 & T3 • T4 & T3 bind to TBGs (thyroid binding globulins – transport proteins in the blood) produced by the liver • Then, T4 & T3 bind to target receptors in various tissues • T3 binds more avidly & is 10x more active • Most tissues have enzymes to convert T4 to T3 • Falling thyroxine blood levels trigger the release of TSH, and ultimately, thyroxine
Hyposecretion of T4 & T3 • BMR rate below normal • Decreased body temperature/cold intolerance • Decreased appetite; weight gain • Decreased glucose metabolism • Elevated cholesterol/triglyceride levels • In infants: • Slowed/deficient brain development, retardation • Growth retardation, retention of child’s body proportion • In adults: • Mental dulling, depression, paresthesias, memory impairment, hypoactive reflexes • Decreased efficency of pumping action of the heart • Low heart rate and low blood pressure • Sluggish muscle action/cramps • Depressed GI motility, constipation • Depressed ovarian function • Sterility • Depressed lactation • Skin pale, thick, dry facial skin, coarse and thick hair
Hypersecretion of T4 & T3 • BMR above normal • Increased body temperature and heat intolerance • Increased appetite & weight loss • Loss of muscle mass • Irritability, restlessness, insomnia, personality changes • Rapid heart rate and palpitations, high blood pressure • Dangerous condition – can lead to heart failure • Muscle atrophy and weakness • In children: accelerated long bone growth but then early epiphyseal plate closure & short stature • Excessive GI motility, diarrhea • Depressed ovulation • Skin flushed, thin, and moist, hair is fine & soft, nails soft & thinning
Calcitonin • Polypeptide hormone produced by parafollicular cells • Lowers blood calcium • Direct antagonist to parathyroid hormone (PTH) which raises blood calcium • Targets the skeleton • It inhibits osteoclast activity • Stimulates calcium uptake and incorporation into the bone matrix • Excessive blood calcium (over 20%) act as a humoral stimulus for calcitonin release • An extremely rapid process • In children, calcitonin plays important role when skeleton is growing quickly • In adults – weak hypocalcemic agent
Parathyroid Glands • Usually 4 glands on the posterior aspect of the thyroid gland • The parathyroid’s glandular cells are arranged in thick branching cords containing oxyphil cells and large numbers of chief cells • Chief cells – secrete PTH – parathyroid hormone • PTH – protein hormone • Triggered by falling blood calcium levels • Inhibited by hypercalcemia • 3 target organs • Skeleton, kidneys & intestines
PTH • Stimulates osteoclasts to digest some bony matrix to increase blood calcium concentration • Enhances reabsorption of calcium by the kidneys • Increases absorption of calcium by intestinal mucosal cells • Enhanced by PTH’s vitamin D activation – better calcium absorption • For Vitamin D to work, the kidneys must turn it into calcitriol – this is stimulated by the production of PTH • Stable calcium levels are important for: • Nerve impulses, muscle contractions, blood clotting • Hyposecretion: tetany, spasms of the larynx, respiratory paralysis, death
Adrenal (Suprarenal) Glands • Pyramid shaped organs perched atop the kidneys – cushioned in fat • Two glands in one • Adrenal medulla – more like nervous tissue than a gland • A part of the sympathetic nervous system • Adrenal cortex – bulk of glandular tissue • Encapsulates the medulla • Medulla & cortex produce different hormones • Both sets of hormones help cope with “extreme” (stressful) situations • Adrenal glands
Adrenal Cortex • Synthesized from cholesterol – about 24 steroid hormones are collectively called corticosteroids • Mineralocorticoids • Regulation of electrolyte concentration (mineral salts: sodium & potassium) • Sodium is essential for homeostasis • Excessive sodium intake and retention cause high BP • Aldosterone – 95% mineralocorticoids produced • Maintaining sodium balance is primary goal • Reduces excretion of sodium from body • Target: distal tubules of kidneys – stimulates reabsorption of sodium ions from forming urine into the bloodstream
Aldosterone • Aldosterone also enhances sodium reabsorption from perspiration, saliva & gastric juice • Crucial for maintaining normal blood flow & BP • Aldosterone’s effects are brief (about 20 mintues) • Therefore, electrolyte balance can be precisely controlled and monitored continually • Secretion stimulated by: • Rising blood levels of potassium • Decreasing blood volume • Decreasing BP • Reverse conditions inhibit aldosterone secretion
Aldosterone • Hypersecretion: aldosteronism: results from adrenal neoplasms • Neoplasms = growths (both malignant & benign) • Problems that arise: edema, accelerated excretion of potassium ions • Extreme potassium loss – neurons are unresponsive, muscle weakness/paralysis may occur • Hyposecretion: Addison’s disease • Results from deficient mineralocorticoid & glucocorticoid release
Regulation of Aldosterone • Renin-angiotensin system • Major regulator of aldosterone • Specialized cells in the kidneys become “excited” when blood pressure/blood volume drops • Kidneys release renin into the bloodstream • Renin reacts with angiotensinogen • Triggers an enzymatic cascade reaction to produce angiotensin II • Angiotensin II stimulates aldosterone to be released by the adrenal cortex • Angiotensin II has widespread effects on BP • Plasma concentrations of sodium & potassium • Increased potassium & decreased sodium are stimulatory • Opposite conditions are inhibitory
Regulation of Aldosterone • ACTH • Under normal circumstances ACTH has little to no effect on aldosterone release • SEVERE STRESS: hypothalamus secretes CRH (corticotropin- releasing hormone) • This steps up the secretion of aldosterone a little • The rise in blood pressure/volume helps ensure adequate delivery of nutrients and respiratory gases during the stressful period • ANP (Atrialnatriuretic peptide) • Natriurietic = produce salty urine • Hormone secreted by the heart • Fine tunes blood pressure and sodium/water balance • Major effect: inhibits renin-angiotensin mechanism • Overall effect – decrease blood pressure by allowing sodium * water to flow out of the body in urine
Glucocorticoids • Influence metabolism of most body cells & help resist stressors • Normal circumstances: help body maintain fairly constant/stable sugar levels when food intake is intermittent • Also maintains blood volume by preventing water shifting into tissues • Severe stress (such as hemorrhage, infections, physical/emotional trauma) • Dramatically higher output of glucocorticoids – help body negotiate crisis • Cortisol, cortisone & corticocosteroneare glucocorticoids • Cortisol is secreted in most significant amounts
Glucocorticoid secretion • Cortisol release is triggered by CRH, which promotes ACTH release • Rising cortisol levels inhibit CRH release and shut off ACTH • Cortisol bursts happen in a regular pattern daily • Based on eating and activity patterns • Peak shortly after waking in the morning, lowest just before sleep and shortly after sleep ensues • Sympathetic nervous impulses can override inhibitory effects of rising cortisol levels • The resulting increase in ACTH causes an outpouring of cortisol from the adrenal cortex.
Stress & Glucocorticoids • Stress results in dramatic rise in glucose, fatty acids & amino acids – all provoked by cortisol • Primary metabolic effect – gluconeogenesis • Creation of glucose from non-carbohydrate molecules • To “save” glucose for the brain, cortisol mobilizes fatty acids from adipose tissue and encourages use for energy • Enhances epinephrine’s vasoconstrictive effects • Rise in BP & circulatory efficiency helps ensure nutrients are delivered quickly to cells
Glucocorticoids • Ideal amounts of glucocorticoids promote normal function • However: • Excessive glucocorticoids: • Depress cartilage and bone formation • Inhibit inflammation & prevent vasodilation • Depress the immune system • Promote changes in cardiovascular, gastrointestinal and neural functioning
Hypersecretion & Hyposecretion • Hypersecretion helps treat chronic inflammatory diseases like RA, or allergic responses • May relieve some symptoms, also causes undesirable effects • Cushing’s disease: • Causes: ACTH tumor in pituitary, malignancy in lungs, pancreas, kidneys or tumor of the adrenal cortex • Most often: pharmacological doses of glucocorticoids (steroids) • Characterized by persistent hyperglycemia, dramatic loss in muscle mass, water/salt retention, leading to hypertension & edema • Hyposecretion: Addison’s disease • Weight loss, glucose & sodium levels drop & potassium rises • Severe dehydration & hypotension is common