Download

1 / 25
250 likes | 520 Views
Visual field defects. The Normal visual field is defined as “ Island of vision surrounded by a sea of blindness ”

E N D
The Normal visual field is defined as “Island of vision surrounded by a sea of blindness” • The three dimensional concept can be reduced to quantitative values by plotting lines (isopters) at various levels around the island or by measuring the height (sensitivity) at different points within the island of vision.
The normal extent of field of vision • 60°nasally. • 50°superiorly • 70°inferiorly . • 90° temporally
common causes of VF defect • Central field loss occurs with: • Optic neuropathy • Macular degeneration • Macular hole • Cone dystrophies • A number of rare conditions like Best’s disease, Stargardt's disease and achromatopsia.
Peripheral field loss occurs with: • Retinitis pigmentosa • Chorioretinitis • Glaucoma • Retinal detachment • Leber's optic atrophy
Assessing for visual field defects can be via • Screening tests… • confrontational visual field testing • Amsler grid (assesses the central 10° the visual field ) . • Quantitative measurements using manual or automated perimetry.
Visual acuity tests the eye's greatest power of resolution . • visual field testing measures the peripheral sensitivity.
Terms • Visual field defect - a portion of visual field missing. This may be: • central (e.g. optic disc or nerve problem) • peripheral (along the visual pathways from the optic chiasm back).
Scotoma - this is a type of visual field defect. It is a defect surrounded by normal visual field. • Relative scotoma - an area where objects of low luminance cannot be seen but larger or brighter ones can. • Absolute scotoma - nothing can be seen at all within that area.
Hemianopia - binocular visual defect in each eye's hemifield. • Bitemporal hemianopia - the two halves lost are on the outside of each eye's peripheral vision, effectively creating a central visual tunnel. • Homonymous hemianopia - the two halves lost are on the corresponding area of visual field in both eyes, i.e. either the left or the right half of the visual field.
Altitudinal hemianopia - refers to the dividing line between loss and sight being horizontal rather than vertical, with visual loss either above or below the line. • Quadrantanopia - is an incomplete hemianopia referring to a quarter of the schematic 'pie' of visual field loss. • Sectoral defect - is also an incomplete hemianopia
Static perimetry • the most commonly used assessment . • An 'on/off' light signal is presented throughout the patient's potential visual field and the patient clicks every time they see the signal. • can assess various amounts of the visual field (10° to full field). • sensitive tests but are difficult to perform • Humphries' (and to a lesser extent, Henson's) machines are most commonly used.
Kinetic perimetry • This presents a moving stimulus from a non-seeing area to a seeing area. • The most commonly used kinetic test is Goldmann perimetry. • It is repeated at various points around the clock and a mark is made as soon as the point is seen. These points are then joined by a line (an isoptre).
Lesions before the chiasm • These will produce a field deficit in the ipsilateral eye. • Field defects from damage to the optic nerve tend to be central, asymmetrical and unilateral. • Lesions just before the chiasm can also produce a small defect in the upper temporal field of the other eye
Lesions at the chiasm • These classically produce a bitemporal hemianopia. • If they spread up from below, for example, pituitary tumours, the defect is worse in the upper field. • If the tumour spreads down from above , e.g. craniopharyngioma, the lesion is worse in the lower quadrants.
Lesions after the chiasm • These produce homonymous field defects. • A lesion in the right optic tract produces left visual field defect. • Lesions in the main optic radiation cause complete homonymous hemianopia without macular sparing. • Lesions in the temporal radiation cause congruous upper quadrantic homonymous hemianopia commonly with macular sparing.
Lesions in the parietal radiation (rare) cause inferior quadrantic homonymous hemianopia without macular sparing. • Lesions in the anterior visual cortex (common) produce a contralateral homonymous hemianopia with macular sparing . • Lesions in the macular cortex produce congruous homonymous macular defect • Lesions of the intermediate visual cortex produce a homonymous arc scotoma, with sparing of both macula and periphery.
Occipital lobe lesions • If both occipital lobes are injured then the patient is in a state of cortical blindness. • some patients deny their blindness and attempt to behave as if they have vision. This state of denial of cortical blindness is called Anton's syndrome.
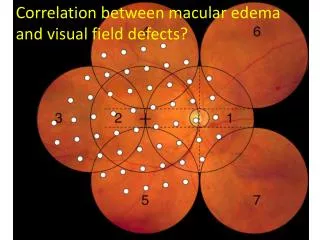
Influence of Glaucoma on Visual Function • The visual field defects that are caused by loss of retinal nerve fiber bundles are the most common and familiar change, the central vision is typically one of the last region to be lost
Visual Field defects in Glaucoma • Arcuate defect • Nasal step • Vertical step • Temporal sector defect
Advanced Glaucomatous Field Defects • Complete double arcuate scotoma with extension to peripheral limits in all areas except temporally • This results in a central island and a temporal island of vision in advanced glaucoma
Disease causing it : 1) Chronic progressive simple glaucoma ( AOG & Chronic ACG ) 2) Advanced retinitis pigmentosa . 3) CRAO with cilioretinal artery . 4) Post-papolloedemic optic atrophy . • Diagnostic for advanced case of glaucoma
Arcuate scotoma , Ronne nasal step & concentric contraction of central field in case of glaucoma