Download
1 / 53
540 likes | 716 Views
Multimodality Conference Testicular cancer. Nagendra Natarajan MD, MPH Fellow – Medical Oncology August 12 2010. Development of Testes. Genotype of embryo (46,XX or 46,XY) is established at fertilization Weeks 1-6, embryo is sexually indifferent/ undifferentiated

E N D
Multimodality ConferenceTesticular cancer Nagendra Natarajan MD, MPH Fellow – Medical Oncology August 12 2010
Development of Testes • Genotype of embryo (46,XX or 46,XY) is established at fertilization • Weeks 1-6, embryo is sexually indifferent/ undifferentiated • This indifferent embryo begins phenotypic sexual differentiation during 7th week of development • By week 12 sexual characteristics of external genitalia can be recognized
Development of Testes • By week 20 phenotypic differentiation is complete • Results in one of the following: • Female phenotype • Male phenotype • Intersex phenotype
Embryogenesis • The components of indifferent embryo that are remodeled to form reproductive system • Gonads – ovaries or testes • Genital ducts – Paramesonephric (female), mesonephric (male) • Primordia of external genitalia
Relative descent of testes • The testes originally develops in the abdomen – later descends into the scrotum • Initial decent to the inguinal canal is due to disproportionate growth of the upper abdominal region away from the pelvic region • Factors involved in the final descent to the scrotum – increased pressure due to abdominal viscera, the gubernaculum and testosterone
Function of testes Two main functions • Formation, development and excretion spermatozoa • Production of testosterone
Structure • Oval – 4 cm long • Outermost layer is formed by dense fibrous membrane called tunica albuginea – collagen and elastic fibers • In the most posterior part of the testis the tunica albuginea extends into the testis – mediastinum testis, dividing the testis into lobules • Each lobule consists of highly convoluted seminiferous tubules (70-80 cm in length)
Structure • Lobules – 200/testicle • Seminiferous tubules - 2 to 3/lobule • Between seminiferous tubules is the very loose connective tissue – blood vessels and lymphatics • Groups of interstitial cells (leydig cells) are present in the connective tissue and these produce the male sex hormone
Germ cells • Germ cells are located in the wall of the seminiferous tubules • These cells are responsible to proliferate and differentiate into spermatocytes • In-between the germ cells are the supporting cells – cells of sertoli
Normal adult testis is shown here at low power, with tubules and intervening interstitium with Leydig cells Normal testis - Histology
Normal testis - Histology • Normal adult testis seen microscopically at high power, with tubules containing prominent spermatogonia maturing to spermatozoa
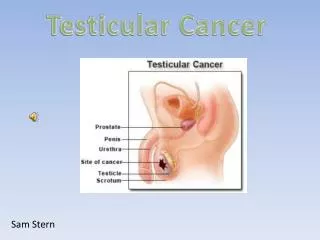
Introduction • Cancers of the testis comprise a morphologically and clinically diverse group of neoplasms, most of which are germ cell tumors (GCTs) • 90% of GCTs originate in the testis • 10% of GCTs are extragonadal – mediastinum, abdomen, pelvis or brain
Extragonadal GCT • The first hypothesis - Abnormal migration of the primordial germ cells • Abnormality in the primordial germ cell itself • Abnormality in its microenvironment
Extragonadal GCT • The second hypothesis is that germ cells transformed in the testes undergo reverse migration • This hypothesis is supported by genetic data suggesting that extragonadal GCTs and testicular GCTs share a common cell of origin
Epidemiology • Median age at diagnosis - 34 years • Age adjusted incidence is 5.4/100,000/year • Lifetime risk of developing testicular cancer is 0.37% • Estimated new cases for 2010 – 8,480 • Estimated deaths for 2010 – 350 • GCTs are the most common solid tumors in men between the ages of 15 and 35 years
International incidence • Highest reported incidence in Scandinavia, Switzerland, and Germany • Intermediate in the United States and Great Britain • Lowest in Africa and Asia
Non GCT’s of testes • Leydig cell tumors • Sertoli cell tumors • Granulosa cell tumors • Gonadoblastoma – common in patients with chromosomal abnormalities and dysgenic gonads • Mesothelioma – arises from tunica vaginalis • Sarcoma – peritesticular and spermatic cord soft tissue • Adenocarcinoma of the rete testis – highly malignant • Lymphoma – most common secondary tumor • Epidermoid cyst • Metastatic carcinoma – rare, most commonly from prostate, kidney, melanoma and lung
Risk Factors Definitive evidence • Cryptorchidism • Inguinal hernia • HIV • Klinefelter syndrome • Testicular dysgenesis • Prior history of GCT • Family history of GCT Tentative evidence • Birth weight • Gestational age Int J Epidemiol. 2010 Jul 26
No association • Vasectomy • DES exposure • Trauma • Viral infection
Symptoms • Painless testicular mass • Discomfort – lower abdomen or scrotum • Lower back pain and discomfort • Urinary difficulty • Scrotal swelling
Workup • If symptoms suggestive of infection – trial of antibiotics is warranted • If symptoms persist – USG of the testis is performed • If intratesticular mass is identified • Beta - hcg • LDH • AFP • Chest X ray
Seminoma Classic (typical) Spermocytic Syncytiocytotrophoblastic Non seminoma Embryocarcinoma Choriocarcinoma Yolk sac tumor Teratoma Mixed germ cell tumor GCT classification
Molecular biology Testicular GCT are invariably aneuploid Gain of the chromosome arm 12p is a consistent finding with testicular GCT This has also been described in GCT’s which arise in cells other than testes Amplification of subregions of 12p at 12p13 and, more frequently, 12p11.2-p12.1 have been described in the absence of isochromosome 12p Lancet 2006; 367: 754–65
Molecular biology Genes including KRAS2, EK11 and LDH B have been identified - amplified and over expressed Examples of genes at 12p13 that encode proteins that could be involved in TGCT development include CCND2 (cell cycle regulation), and NANOG and STELLAR (maintenance of pluripotency in stem cells) Lancet 2006; 367: 754–65
Molecular biology CGH and allelic imbalance studies have shown that several other regions of the genome are also imbalanced, at a lower frequency than the gain of 12 p Microarray analyses have defined regions more precisely such as gain of material from the regions 4q12, 17q21.3, 22q11.23, and Xq22 and loss from 5q33, 11q12.1, 16q22.3, and 22q11 Lancet 2006; 367: 754–65
Molecular biology The KIT gene at 4q12 encoding a tyrosine kinase receptor amplified and overexpressed in some seminomas Other evidence supporting a role for KIT in seminomas is activating mutations in the gene with a reported higher frequency in bilateral cases Activating mutations in K- and N-RAS have been described in both seminomas and non-seminomas Lancet 2006; 367: 754–65
Molecular biology of therapy The molecular basis of germ-cell transformation, differentiation, and the extreme sensitivity of GCT to cisplatin therapy is poorly understood Studies have shown that TGCTs are 2-4 fold more sensitive to chemotherapeutic agents and irradiation than other types of cancer cells Lancet 2006; 367: 754–65
Molecular biology of therapy Factors that influence cells’ response to therapeutic agents Processes affecting the drug’s influx and efflux Metabolism of the drug by the cells Accessibility of the drug to DNA Cell response to DNA damage No differences between TGCT and other cancer cells have been identified in terms of these factors Lancet 2006; 367: 754–65
Molecular biology of therapy Elevated levels of wild-type p53 in TGCT could activate an apoptotic response to DNA damage However, uniform overexpression is not found and mutation in p53 does not necessarily correspond to resistance TGCTs are deficient in nucleotide excision repair and might have other repair defects. This, combined with the TGCT cells’ ability to respond to damage by apoptotic mechanisms, could contribute to their unique sensitivity Lancet 2006; 367: 754–65
Seminoma • 50% of GCT • Fourth decade of life • The typical or classic form consists of large-cell sheets with abundant cytoplasm, and round, hyperchromatic nuclei with prominent nucleoli • Lymphocytic infiltrate (and/or granulomatous reaction with giant cells) is frequently present
Seminoma • Histological classification • Classic (Typical) • Spermatocytic, rare, older men, better prognosis • Syncytiocytotrophoblastic associated with increased Beta-hcg levels
NSGCT • 50% of GCT • Third decade of life • Most tumors are mixed
NSGCT • Embryonal carcinoma • Yolk sac tumor • Choriocarcinoma • Teratoma – mature, immature and malignant transformaton • Mixed GCT
Serum tumor markers • α-Fetoprotein • Β – HCG • LDH
α-Fetoprotein • AFP is determined by a two-site immunozymatic assay using World Health Organization (WHO) standard code 72/225, in which 1 IU AFP corresponds to 1.21 ng • The normal adult serum concentration is usually less than 15 ng/mL • Approximately 10% to 20% of clinical stage I, 20% to 40% of low-volume clinical stage II, and 40% to 60% of advanced NSGCT will have increased AFP levels • Increased AFP levels are never seen in pure seminoma. Its serum half-life is 5 to 7 days
Human Chorionic Gonadotropin • HCG, composed of an α and β subunit, is produced by syncytiotrophoblasts • Most commercial methods have adopted the WHO Third International Standard (code 75/537), resulting in some uniformity in immunoassays to detect the HCG β subunit. • Approximately 10% to 20% of patients with clinical stage I, 20% to 30% with low-volume clinical stage II, and 40% with advanced NSGCT present with elevated serum concentrations of HCG. Approximately 15% to 20% of patients with advanced pure seminoma have increased serum concentrations of HCG • The serum half-life of HCG-β is 18 to 36 hours
LDH • Elevated levels reflect • Tumor burden • Growth rate • Cellular proliferation • Increased serum LDH concentrations are observed in approximately 60% of NSGCT patients with advanced disease and up to 80% of patients with advanced seminoma
Non seminoma www.NCCN.org
Non seminoma www.NCCN.org