Download
1 / 25
270 likes | 515 Views
Utilizing Molecular Prognosis in Early-Stage Non-Small Cell Lung Cancer. Title Slide. Disclosure. Life Technologies Corporation (Consultant). Molecular Prognosis in Early-Stage Non-Small Cell Lung Cancer. Objectives Need for better prognostic information in managing early stage NSCLC

E N D
Utilizing Molecular Prognosis in Early-Stage Non-Small Cell Lung Cancer Title Slide
Disclosure Life Technologies Corporation (Consultant)
Molecular Prognosis in Early-Stage Non-Small Cell Lung Cancer Objectives • Need for better prognostic information in managing early stage NSCLC • Immediate clinical utility of improved prognostic differentiation of risk within stages I and II NSCLC • Development of the first practical, well-validated multi-gene prognostic assay for non-squamous, NSCLC (PervenioTM Lung RS) • Research opportunities during the early implementation of molecular prognostic testing in the management of early stage NSCLC
Early-stage lung cancer • AJCC 7th edition staging – introduced in 2009 • Based on anatomic/histologic criteria only • Does not adequately discriminate between patients with different levels of risk • Five-year mortality for patients with pathologic stage I lung cancer is 30-45% • Increasing diagnosis at early stages due to more frequent imaging Detterbeck FC et al. Chest 2009; 136: 260-271.
Poor Early Stage Outcomes • Why do patients with early stage disease have such poor outcomes? • Death-from co-morbidities • Misdiagnosis • Development of second primary tumors • Major culprit: Recurrence due to metastatic disease that must be present but is undetectable at the time of resection Martini et al. J Thorac Cardiovasc Surg 1995
Need for practical, validated molecular prognostic for early-stage lung cancer • Large unmet need for more precise prognostic information in the management of early stage NSCLC • Lung cancer community frustrated by consistently poor outcomes in early stage disease • 30-60% of “early stage” patients die with distant recurrence - metastasis that was present but undetected at the time of surgical resection
Clinical utility of well-validated molecular prognostic for early-stage lung cancer • Stage II • Suboptimal compliance with recommendations for adjuvant therapy in stage II • Relatively small survival benefit has curtailed enthusiasm • Until now, degree of benefit measured in all-comers, without regard to true risk within stage • Largest benefit has been seen in highest risk • Patients now identified as highest risk less likely to forgo therapy
Clinical utility of well-validated molecular prognostic for early-stage lung cancer • Stage I • Given the dismal prognosis, published guidelines already recommend chemotherapy for “high risk” stage I patients • NCCN level 2B recommendation: “there is NCCN consensus that the intervention is appropriate” • Stage IB plus one of six anatomic/histologic criteria • Therapy recommended despite absence of prospective data documenting a benefit • No validation that these “high risk” criteria truly identify those at highest risk
Clinical utility of well-validated molecular prognostic for early-stage lung cancer • Stage I • Default degree of evidence supporting NCCN guidelines for NSCLC is “2A” • “lower level evidence” - no randomized data • Best available information must be synthesized into the best possible recommendation for patients facing grave prognoses with few good choices • Difficult decisions must be made for early stage patients - more accurate prognostic information would lead to more informed decisions
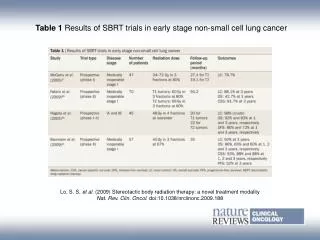
Have molecular assays met this need? Practical, reproducible assay with large-scale, independent validation Table adapted from Subramanian J and Simon R, J Natl Cancer Inst 2010;102:464-74..
paraffin-tissues qPCR blinded Assay Development Measure expression of 14 cancer pathway + reference genes (CLIA-certified Laboratory) L2-penalized Cox Proportional Hazards Modeling 361 stage I-IV non-squamous FFPE samples (UCSF Training Cohort) Prognostic Algorithm Kaiser Northern California 433 stage I samples Analytical Assay Validation (CLIA-certified Laboratory) Independent Clinical Validations China Clinical Trials Consortium 1006 stage I-III samples
Assay Overview Lung Cancer Sample (Formalin-Fixed Paraffin Embedded Blocks) Block Sectioning Paraffin Slices mRNA Extraction mRNA Reverse Transcription cDNA Quantitative Real-Time PCR mRNA quantification Prognostic Algorithm Identify HIGH risk patients
The Lancet University of California, San Francisco, CA, Department of Cardiothoracic Surgery, The First Affiliated Hospital of Guangzhou Medical College, State Key Laboratory of Respiratory Disease, Guangzhou, China Kaiser Permanente Dept of Research, Northern California, Oakland, CA, Department of Thoracic Oncology, Cancer Centre of Sun Yat-Sen University, Guangzhou, ChinaShanghai Pulmonary Hospital, Shanghai, China Beijing Lung Cancer Centre, Capital Medical University, Beijing, China Pinpoint Genomics, Mountain View, CA
China Clinical Trials Consortium (CCTC): Bridging East and West • Peking University Medical College • Capital University of Medicine • Tianjin Cancer Center • Shanghai Pulmonary Hospital • Shanghai Chest Hospital • Huaxi Hospital: • 5,000 beds • Guangzhou Medical College • Sun Yat-sen Univ. Cancer Center • Clinical Sites • Strategic Laboratories • Multiple Cancer Specialties • Lung, Breast, Colorectal, Prostate, Liver
Only practical, validated molecular prognostic for early-stage lung cancer • Large-scale validation studies: ~1,500 Patients China Clinical Trials Consortium: 1006 patients (Stages I-IIIa) Kaiser Northern California: 433 patients (Stage I) Kratz et al. Lancet 2012;379:823 .
Only practical, validated molecular prognostic for early-stage lung cancer • Large-scale validation studies: China Clinical Trials Consortium: Stage II (222 patients) China Clinical Trials Consortium: Stage I (471 patients) Kratz et al. Lancet 2012;379:823 .
Only practical, validated molecular prognostic for early-stage lung cancer Large-scale validation studies: • Molecular assay outperformed NCCN criteria for identifying “high risk” stage I patients • Kaiser Northern California (Stage I): Multivariate Analysis Kratz et al. Lancet 2012;379:823 .
Only practical, validated molecular prognostic for early-stage lung cancer Large-scale validation studies: • China Clinical Trials Consortium (Stage I-III): Multivariate Analysis • Scale of validation similar to validation of new TNM stage I Kratz et al. Lancet 2012;379:823 .
Genetic Assay Outperforms Conventional Methods Multi-Gene Assay vs. Conventional Staging Multi-Gene Assay vs. NCCN Guidelines China Kaiser
Only practical, validated molecular prognostic for early-stage lung cancer Large-scale validation studies: • Discrimination even of high risk patients with < 2 cm, node negative tumors ….JAMA January 2013 presented at STS
Summary • There is a need to improve NSCLC staging beyond conventional morphologic criteria • A robust, practical assay prognostic of survival after resection has been developed using qPCR and paraffin-tissues • This multi-gene assay has been independently validated in the two largest international cohorts ever studied in the molecular analysis of NSCLC - on a scale similar to that used for validation of stage I of the new TNM system (AJCC 7th edition) • The multi-gene assay can outperform conventional risk factors / staging for patients with early stage non-squamous NSCLC
Only practical, validated molecular prognostic for early-stage lung cancer Conclusions • Conventional staging does a poor job of stratifying risk in early stage NSCLC compared to other common solid tumors • As a result many patients (30-60%) harbor unsuspected metastatic disease after resection but forgo any early systemic intervention • Clear evidence exists that some patients with early, likely micro-metastatic NSCLC will benefit from adjuvant chemotherapy - Improved, and not just prolonged, survival in adjuvant studies - Greatest benefit observed among patients at greatest risk
Only practical, validated molecular prognostic for early-stage lung cancer Conclusions • The default level of evidence supporting NCCN recommendations for NSCLC is 2A (no randomized data) • Given the grave prognosis, even in stages I and II, guidelines already recommend adjuvant therapy for highest-risk patients – even in the absence of prospective outcomes data (Stage I) • Difficult decisions regarding post-operative management are being made now with suboptimal prognostic data – better data will likely lead to better decisions
Diagnosis & Surgery Adjuvant Therapy Chemotherapy/ Palliative Care Monitoring Monitoring Recurrence? Recurrence? Changing the Treatment Paradigm Current Treatment Paradigm Monitoring First-Line Therapy Continued Therapy Diagnosis & Surgery Recurrence? Recurrence? TIME Treatment Paradigm with molecular prognostic testing — + Low Risk Molecular Test High Risk — +
PervenioTM Lung RSProspective Trial: Improvement in Survival in High Risk Stage I Patients • 4 cycles cisplatin doublet • Routine CT scans • DFS • OS PervenioTM Lung RS Prognostic Analysis Chemotherapy Randomization High Risk Observation Molecular Prognostic analysis: R0 resection Non-squamous NSCLC Pathologic stage I Intermediate Risk • Routine CT scans • DFS • OS Excluded Low Risk Observation