Download
1 / 20
200 likes | 458 Views
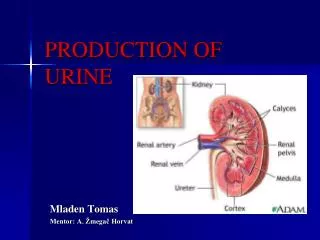
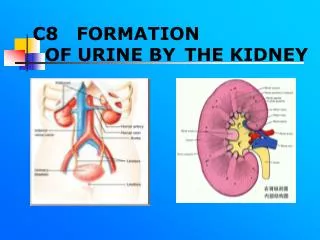
Pathobiochemistry of kidney. Pathological components of urine. PROPERTIES OF URINE Amount – 1500-2000 mL/day Poliuria – diabetes mellitus and insipidus Oliguria – heart failure, nephritis, vomiting, fever Anuria – kidney failure, acute intoxication by heavy metals

E N D
Pathobiochemistry of kidney. Pathological components of urine.
PROPERTIES OF URINE Amount – 1500-2000 mL/day Poliuria – diabetes mellitus and insipidus Oliguria – heart failure, nephritis, vomiting, fever Anuria – kidney failure, acute intoxication by heavy metals Color – straw-yellow Pale – poliuria (diabetes insipidud) Dark – jaundice, concentrated urine Red – blood available Green-blue – decay of proteins in the intestine Transparency – transparent Cloudy – pus or mucin available
Density – 1,003-1,035 g/mL Increased density – organic or inorganic substances available (diabetes mellitus) Decreased density – diabetes insipidus Isostenuria – continuously low density in oliguria (kidney failure) pH – 5.5-6.8 Acidic – meat food,diabetes mellitus, starvation, fever Alkaline – plant food, cystitis, pyelitis
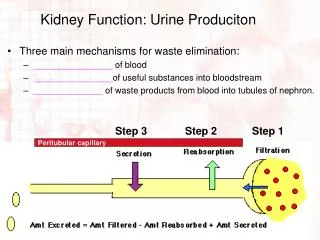
Filtration disorder • Glomerules filtration processis possible to consider aswater and molecules pushing through sieve under infuence of arterial pressure in a remote capillary • This passive process depends on • hydrostatic exacter • filtration pressure, which displace a liquid part fromcapillary blood into a canaliculus lumen of and does not requireenergy • Filtrational pressure, which predetermines glomerules filtrate derivation, is equal to 15-25 mm Hg • In case such filtrational pressure in healthy person Broumen capsula 120 ml of filtrate per 1 mines is derivated, that is 180 l per one day • The glomerules filtation can be decreased or increased
Reason of filtration decrease: • 1.Hydrostatic pressuredecrease inglomerules capillaries:in general decreasing of arterial pressuredecrease (heart insufficiency, shock, collapse, hypovolemia),narrowing glomerules afferent arterioles(arterial hypertension, pain): aorta and kidneys arteries organic defeats (aorta coarctation, stenosic aorta atherosclerosis due to hypertonic illness), kidneys arteries thrombosis or embolism • 2.Plasma oncotic pressureincrease – protein blood substitutes transfusion in large volumes • 3.Intrakidney pressureincrease – canalicules block with cylinders or urinary tract with stones • 4.Glomerulus filterdisorder – quantity functioning glomerulus decrease, glomerulus a membranethickening, an pores amount and diameterdecrease, basal membrane glycoproteid components autoallergic defeat
The most characteristic manifestations of filtration limitation in glomerules are: • nitrogenemia (accumulation in blood of nitrogen metabolic and blood residual nitrogen increase) • renal nitrogenemic acidosis owing to delay in an organism phosphates, sulfates and organic acids • Increase of filtering performs resulting blood pressure increase excessive consumption water, decomplication edema or oncotic plasma pressure decrease (hepatitis, cirrhosis) • Major increasedglomerulus filter permeability manifestations concern: • proteinuria –evacuation with urine of plasma proteins over physiological norm (30-80 mg/day) and in urine protein fractions appearance with molecular weight more than 70 kD • hematuria – erythrocytes kidneys outlet in canalicules lumen of and their appearance.
Reabsorption disorder • The daily ultrafiltrate amount, which gets into canalicules makes equal 99 % of this volume is exposed to a converse absorption mainly in proximal canalicules • Reabsorption proteins, glucose, aminoacids, electrolytes, bicarbonates, phosphates and wateralmost completelyare exposed • Thereabsorbtion selectivity provides kidneys epithelium ability to reabsorp one substance and simultaneously prevents the other. This function is executed by specific molecules – which are the carriers • The dependence of reabsorbtion processes on moleculesmembrane – carriers means the limited canaliculus epithelium ability to transport reabsorbed substance • If the concentration of substance in glomerulus filtrat exceeds possibilities transport system, then given substancethreshold exceeding • Takes place maximal reabsorption substrate speed is named as a maximal tubular one
Disorder of the canalicules functionis called as tubular insufficiency • It can be hereditary or acquired • The selective disorders reabsorption of separate ultrafiltrate components are convenient to separate considering • Disorder sodium and water reabsorbtion • The increase of reabsorption is observed in fallowing case: hyperaldosteronism, oliguri stage of acute kidney insufficiency, reabsorption decrease – hypoaldosteronism, diabetes insipidus • Sodium and water reabsorption is decreased as a result of canalicules epithelium metabolism inhibition by some poisons, including medicines, in particular, mercury diuretics. Reabsorbtion is limited because of glomerulus filtrate osmotic active substances (glucose, urin), increase owing to that so-called osmotic diuresis arises (example, diabetes mellitus) • The heavy disorders of sodium and water resorbtion arise in case dystrophic and inflammatory canaliculus epithelim changes, so canalicules lose the ability to liquid concentration and cultivation. Loss of concentration ability is called hypostenuria, relative density aqual in state changes within the limit of 1,006-1,012 (norma – 1,002-1,035). If density urine is kept at 1,010level and is not changed with influence water load, it is calledisostenuria (monotone diuresis)
The disorder of proteins reabsorption appears as tubular proteinuria • It is observed due to poisoning cadmium, hypoxia, burns, septicemia • Moderate tubularinsufficiency is characterized by the rather low contents in urine of albumins and other proteins with weight up to 40 kD (selective proteinuria). Dystrophic defeats canaliculuslead to in urine appearence proteins with molecular weight more than 40 kD (unselective proteinuria)
The disorder of reabsorbtion proteins appears as a tubular proteinuria • It is observed in case cadmium poisoning, hypoxia, burns, septicemia • Moderate tubular in sufficiency is characterized by rather albumins and other proteins with weight up to 40 kD is characterized in urine (selective proteinuria) • In case of rougn dystrophic canaliculuc defeats, there are proteins in urine with molecular weight more 40 kD (unselective proteinuria)
The glucose reabsorbtion disorders Dayly norm of glucose loss with urine- up to 1g There are renal and extrarenal glucosuria. • Renal glucosuria arises as a result : • Hereditary anomalia membrane carriers deficiency enzymes hexokinase and glucose-6-phosphatase, which provide glucose canalicules reabsorption. • Equired decrease of these enzymes activity in case of chronic poisonings with lead, mercury, uranium compounds. • Experimentally it is possible to resynthesis by means of floridsine,which oppresses phosphorilation in canalicules cells. • Extrarenal glucosuria stipulated hyperglycemia which exceeds renal threshold (9.0 – 10 mmol/l). More often it is observed due to diabetes mellitus.
The inorganic phosphate and calcium disorder reabsorbtion have the hereditary character. • Renal phosphate diabetes is manifested with phosphaturia, calciuria, rachitis, resistance to vitamin D, canalicules sensitiviby to parathormone increase (pseudohyperparathyroidism). • Hereditary osteodystrophias are characterized with hypocalciemia, hypophosphatemia, parathormone canalicules resistance because of appropriate receptors absence ( pseudohyperparathyroidism) • The aminoacids reabsorbtiondisorder causes aminoaciduria. • Renal aminoaciduria develops due to of the normal aminoacids contents in blood and is explained by hereditary transport or membrane molecules-carriers deficiency. • Extrarenal aminoaciduria is observed in case of increase catabolism proteins (disintegration tumor, inflammation), phenylketonuria, cystinosis, hyperglycinemia
Combined tubulopathia. • The most known example of suchdisorders is the Fankony syndrome. • In basis of this symptomocomplexlies kidneys canalicules function generalized disorder. • Itincludes glucosuria, aminoaciduria, phosphaturia, hypercalciuria, hypernatriuria, proteinuria, proximal renal canalicules acidosis with bicarbonaturia, rachitis with resistantion to vitamin D. Disoder of secretion • The main manifestation – canaliculus acidosis; ammonium- and acidogenesis inhibition and secretion H+-ions lies it is basis. Hyperuricemia, which develops owing tourinary acid secretiondisorder and lead to gout (renal form). • Kidneys functionsdisordersof can be completed with their insufficiency.
Chronical renal insufficiency (CRI) Symptoms chronical renal insufficiency develops in case GFS 25 % over norm • The main reasons: • primary glomerulus diseases (chronic glomerulonephritis) • the primary canaliculus diseases (chronic pielonephritis tuberculosis) • vascular diseases (hypertonic illness, thrombosis, embolism) • diffuse connective tissue diseases (sclerodermia, nodular periarteriitis) • illness metabolism (gout, diabetes mellitus), • obstructive nephropathia(urolithiasis, hydronephrosis), hereditary anomalies ( kidneys polycystic)
Renal functions decrease occurs due to decrease of functionnephronsamount acting nephrons • The initial chronical renal insufficincy signs occur owing to mass of acting nephrons decrease to 50-30 % • The expressed clinic developsdue to acting nephronsdecrease down to30-10 % • Further actingnephronsweight decrease (is lower than 10 %) results in terminal kidneys insufficiency stage – uremia
Decrease of phosphatesexcretion lead to increase their level in blood. • Result hydroxiapatite is derivationand ionized calciumlevel is decreased, thus it stimulates parathyroid glands. If GFS falls below 25 % of norm, secondary hyperparathyreosis become obvious. • Resorbtion of bones is increasedand their density is decreased. When weight nephrones is less than 25 %, the 25-ОН-vitamin Dtransformation to the active form – 1,25 (OH)2-vitamin Dtransformation is decelerated. It is the reason of calciumdelay absorbtion in alimentary channel
Uremic encephalopathyappears with sleepiness, inability to concentration, absent-mindness, and then – amnesia, hallutinations, delirium, cramps • These bones change are capable to render destructive action on organism • Delay growthin children in adult bones delaypain fractures, compression vertexos femoris head, necrosis and skeleton deformation • Arterial medial layer calcification can be observed with ischemicnecrosis soft tissue skin calcification with intolerable itch, periarteriitis owing tocalciumoxyapatitis precipitation, calcification
Uremia • Uremia is a term, which is used for chronical renal insufficiency terminal phase description. The majority of symptoms become well expressed in GFS ratio below than 10 ml/min. • Uremic syndrome pathogenesis has become subject of intensive learning for a long time. The numerous attempts were made to identify substances, which are accumulated inrenal insufficiency terminal phase and reach dangerous to the vital function data.
Uremic toxinsis nitrogen metabolismproducts. • They are: urea, guanidine derivatives (methylguanidine, guanidinsuccinic and guanidinacetative acids, kreatine and kreatine), aromatic compounds (phenole, indole, aromatic amines), conjugated aminoacids, lowmolecular peptides. • In uremiadevelopment significance ispeptides hormones accumulation– parathhormone, insuline, glucagone, gastrine, vasopressine, adrenocorticotropic and somatotropic hormones. In the kidneys is catabolysed 25 % of peptide hormones. Some effectsis stipulated compounds deficiency, which are not synthesized due to uremia. Examples – erythropoietine and 1,25-dioxyеnolecalciferoldeficiency.