Download
1 / 31
362 likes | 888 Views
Introduction of antimicrobial. dr. Dina Fauzia , SpFK Bagian Farmakologi dan Terapi Fakultas Kedokteran Universitas Riau Januari 2012. Introduction. Antimicrobial agents are the most commonly used and misused of all drugs.

E N D
Introduction of antimicrobial dr. Dina Fauzia, SpFK BagianFarmakologidanTerapi FakultasKedokteranUniversitas Riau Januari 2012
Introduction • Antimicrobial agents are the most commonly used and misused of all drugs. • The inevitable consequence emergence of antibiotic-resistant pathogens. • Reducing inappropriate AM use is thought to be the best way to control resistance. • Over prescribing remains widespread: • patients demand, • time pressure on clinician, • diagnostic uncertainty
Introduction (2) • Lack of new antimicrobial agents developed in recent years. • Unnecessary financial burden to the patients. • Scarcity of objective information on appropriate use of antimicrobial agents.
Susceptibility and Resistance • If the microorganism is considered to be susceptible to the antibiotic when the drug concentration at the site of infection inhibit ( bacteriostatic effect) or kill ( bactericidal effect ) the themicroorganism. • Inhibitory or bactericidal concentration cannot be achieved safely, then the microorganism is considered resistance to the drug.
Susceptibility of Microorganism to AMA • Successful AM therapy depends on concentration of AMA at the site of infection • must be sufficient to inhibit the growth of microorganism • must remain below toxic level in this condition, microorganism is considered susceptible to AMA. • If host defenses are intact and active, bacteriostatic agent may be sufficient. • If host defenses are impaired, a bactericidal effect is required
Bacterial Resistance to AMA • The emergence of bacterial resistance to AMA is a very serious development that threatens the end of antibiotic era. • For an antibiotic to be effective, it must reach its target, bind to it, and interfere with its function. • Mechanism of bacterial resistance to an antimicrobial agent falls into three general categories: (1) the drug does not reach its target; (2) drug is not active; (3) the target is altered
Pharmacokinetic factors of AM therapy • Most antimicrobial agents and their metabolite are eliminated primarily by the kidneys. • One must be particularly careful when using aminoglycosides, vancomycin, and fluocytocine in patients with impaired renal function. • For AM that are metabolized or excreted by the liver, dosage must be reduced in patient with hepatic failure. • Oral administration is preferred, but parenteral AM is recommended in in seriously ill patients
Selection of AMA • Four options of AM therapy: • Empirical, experimental, definitive, prophylaxis. • Empirical th/ is widely utilized, and is potential for abuse. • Whenever initiate empirical therapy, cultures of the presumed site of infection should be taken prior to the institution of AM therapy. • The location of the infection may usually the choice of drug and the route of administration
Selection of AMA(2) • Considerations in selecting an AMA : • Whether it is even indicated: • Use “educated guess” or • Culture and sensitivity test, if appropriate • In cases of symptoms are present but are not life-threatening, it is better to postpone the AM Th/ until the D/ is obvious. Example: FUO
Selection of AMA (3) • Optimal and judicious selection of AM requires: • clinical judgment • detailed knowledge of pharmacological and microbiological factors • knowledge of the most likely infecting microorganisms and their susceptibility to AMA. • The most practical method for immediate identification of bacteria is examination of the infected secretion or body fluids with Gram’s stain.
Selection of AMA (4) • In many situations, identification of morphology of the infecting organism is not adequate to arrive at specific bacteriological diagnosis Broad spectrum AM is then indicated, Culture of the presumed site of infection and blood, should be taken prior to the institution of drug therapy. • For definitive therapy, once an organism has been isolated and results of susceptibility tests are known, the regimen should be changed to specific and narrow spectrum AMA
Tips for Selecting AMA • If a sensitivity test indicates that a pathogen is sensitive to some antibiotics, it does not mean all these agents are equally effective in clinical setting. • If 2 antibiotics are equally safe and effective, choose the one with narrower antibacterial spectrum. • Generic antibiotics are not of low quality but their price is much more affordable.
Tips for Selecting AMA(2) • Do not use obsolete antibiotics • A new generation antibiotic is not always superior to its older generations • A slightly more potent antibiotic shown in vitro, is not necessarily associated with better clinical efficacy
Antimicrobial Combination INDICATIONS • Severe infection in which the cause is unknown. Prolong use should be avoided, because toxicity, superinfection, and selection of multiple drug resistant may result. • Polymicrobialinfection • To have synergistic effect in specific infection (endocarditis, Ps aeruginosa infection, H influenza infection). • To prevent the emergence of resistant microorganism (in TBC, H pylori infection)
Antimicrobial Combination(2) DISADVENTAGES • Increase risk of toxicity • Selection of multiple-drug resistant microorganisms • Eradication of normal host flora with subsequent superinfection. • Increase cost to patients • Possibility of antagonistic effect.
Role of Host Factors in AMT • The functional state of host defense mechanisms is a critical determinant of therapeutic effectiveness of AMAs. Both humoral and celular immunity are important. • In the immunocompetent host, halting the multiplication of microorganisms with a bacteriostatic agent is sufficient to cure the infection. • In immunocompromized host, a bactericidal agent is required (bacterial endocarditis, bacterial meningitis, infections in neutropenic patients, HIV/AIDS, uncontrolled DM, malnutrition, …)
Role of Host Factors in AMT(2) Local factors affect the AM activity. • Pus, can bind drugs or inhibit drug action. Low pH in infected sites and anaerobic condition can reduce AM activity, particularly aminoglycosides. • Foreign body markedly reduces the likelihood of successful AM therapy. • Prosthetic materials promotes a bacterial biofilm that impairs phagocytosis. Within the biofilm , bacterial density is high and bacterial growth is slow. favor bacterial persistence frequent relapses.
Prophylaxis of Infection with AM • Chemoprophylaxis is used to protect patients from invasion by specific microorganisms to which they are exposed. But it remains controversial in numerous situations. • Features of successful prophylaxis: • Aimed at a specific pathogen • The pathogen is highly sensitive to the prophylactic agent used. • Features of unsuccessful prophylaxis: • Aimed at any or all microorganism in the environment of a patient
Effective and Judicious Use of Surgical Antibiotic Prophylaxis • AMA must be present at wound site at the time of its closure. The drug must be given iv within 1 hour before incision and another one dose intra operatively for prolong procedure. • The AMA must be active against the most likely contaminating microorganisms. • AM must be present at the wound site at the time of its closure.
Effective and Judicious Use of Surgical Antibiotic Prophylaxis (2) • The continued use of AMA after surgical procedure is unwarranted and potentially harmful. • Use beyond 24 hour is unnecessary. • Prophylaxis is justified in dirty and contaminated procedure. • In clean surgery, AMA should not be used routinely.
Duration of AM Therapy Determined by: • The ability of the pathogens to resist host’s defense mechanism • Physical location of the pathogen • Potency of the AM agent • The frequency of development of resistance
Factors causing Failure of Treatment • Poor antibacterial activity of a drug • Wrong route of administration or wrong dosage • The location of infection is inaccessible by the antimicrobial agent • Poor host ‘s defense mechanism • Premature discontinuation of treatment
Factors causing Failure of Therapy(2) • Serious toxicity necessitates discontinuation of therapy • Resistance of the microorganism • Superinfection • Foreign body or necrotic tissues • Patient’s incompliance
Misuses of AMAs (1) • Treatment of viral infections • Therapy of FUO which can mask an underlying infection, delay the diagnosis, prevent identification of the infectious pathogen by rendering culture negative. • Improper dosage, wrong frequency, excessive or subtherapeutic dose. • Inappropriate reliance on chemotherapy alone. Drainage, debridement, and removal of foreign body are important.
Misuses of AMAs(2) • AM for hospitalized patients is too often given in the absence of supporting microbiological data. • Bacterial culture and Gram stains frequently are not available; when available the results often are disregard of the selection and application of drug therapy. • Frequent use of drug combinations or drugs with broader spectra as a cover for diagnostic imprecision. • Routine dosage rather than individualized on the basis of clinical situation, microbiological information, and the pharmacological consideration.
Past strategies That narrow-spectrum agents be used. That agents be used at the minimum doses possible based on clinical trial data. That antibiotic be used for unnecessarily long period of treatment. Net Results Emergence of antimicrobial resistance Past vs New Strategies
Past vs New Strategies(2) • Future strategies • Using more potent (not necessarily broader spectrum) antimicrobial agent • Using more appropriate (perhaps higher) doses and more appropriate (more frequent) dosing interval • Using antimicrobial for appropriate (possibly shorter) duration. • Net Results • Delaying, reducing or reversing the trends toward higher antimicrobial resistance rates
Superinfection • Definition: appearance of bacteriological and clinical evidence of new infection during the AMT of a primary one. • Therapeutic doses of AMA alter the normal microbial population of intestinal, respiratory, and urinary tracts; as a result, some develop superinfection. • Microorganism responsible for the new infection can be drug-resistant strain of enterobacteriaceae, Pseudomonas, and Candida. • The broader the AM spectrum, and the longer the period of AM treatment, the greater is the possibility of superinfection produced by a typical drug-resistant microorganism.
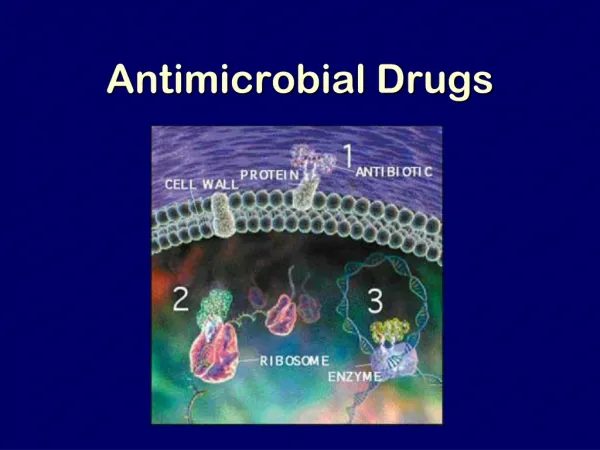
Antimicrobial agents • Antibiotics are substances produced by various species of microorganisms that suppress the growth of other microorganisms • The term antibiotics includes synthetic antimicrobial agents, such as sulfonamides and quinolones
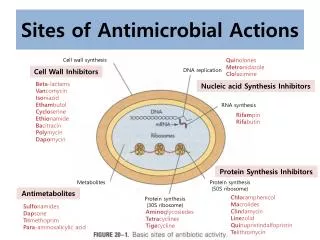
Antibiotic Classification • Classification has been based on chemical structure and mechanism of action: (1) inhibit of cell walls ( penicillins, cephalosporins ); (2) act on cell membrane leading leakage intracellular substances ( amphotericin B, polymixin ); (3) inhibit protein synthesis reversibly ( chloramphenicol, erythromycin); (4) alter protein synthesis leading to cell death (aminoglycosides); (5) affect nucleic acid metabolism ( rifamycins ); (6) block essential enzymes ( sulfonamides, trimethoprim ).