Download
1 / 1
10 likes | 176 Views
Novel Biosignal Parameters Relate To The Brain-Heart Axis Concept In Ischemic Stroke Patients With Atrial Fibrillation: A Preliminary Study Rattapong Sungnoon , MD 1 *, Sombat Muengtaweepongsa , MD 2 , Kesorn Suwanprasert , PhD 2 1 Medical Engineering Program, 2 Faculty of Medicine,

E N D
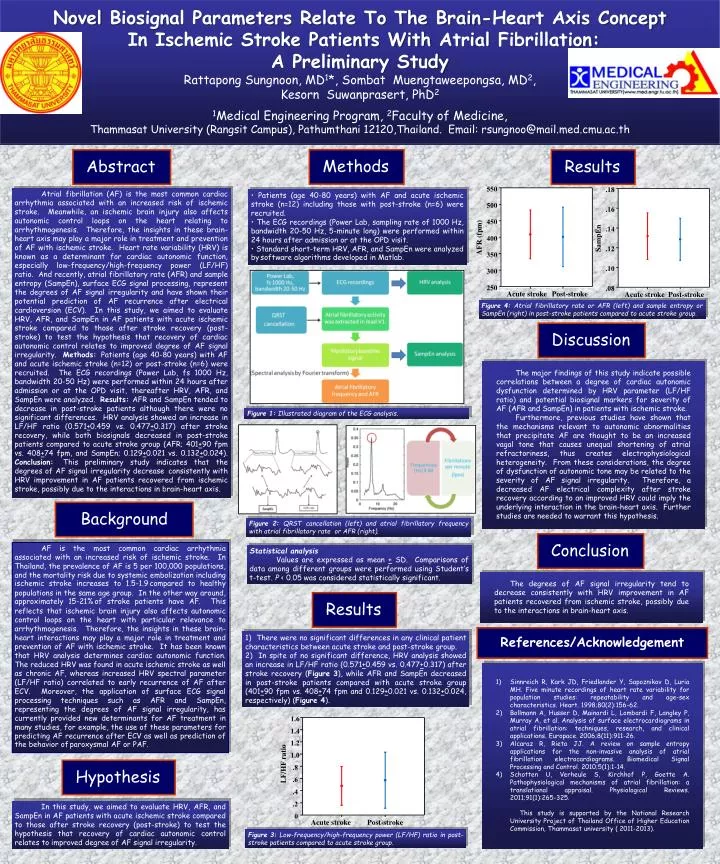
Novel Biosignal Parameters Relate To The Brain-Heart Axis Concept In Ischemic Stroke Patients With Atrial Fibrillation: A Preliminary Study RattapongSungnoon, MD1*, SombatMuengtaweepongsa, MD2, KesornSuwanprasert, PhD2 1Medical Engineering Program, 2Faculty of Medicine, Thammasat University (Rangsit Campus), Pathumthani 12120,Thailand. Email: rsungnoo@mail.med.cmu.ac.th .18 1.6 1.4 .16 1.2 1.0 .14 LF/HF ratio .8 SampEn .12 .6 .4 .10 .2 .08 0 Methods Abstract Results Acute stroke Acute stroke Post-stroke Post-stroke 550 Atrial fibrillation (AF) is the most common cardiac arrhythmia associated with an increased risk of ischemic stroke. Meanwhile, an ischemic brain injury also affects autonomic control loops on the heart relating to arrhythmogenesis. Therefore, the insights in these brain-heart axis may play a major role in treatment and prevention of AF with ischemic stroke. Heart rate variability (HRV) is known as a determinant for cardiac autonomic function, especially low-frequency/high-frequency power (LF/HF) ratio. And recently, atrialfibrillatory rate (AFR) and sample entropy (SampEn), surface ECG signal processing, represent the degrees of AF signal irregularity and have shown their potential prediction of AF recurrence after electrical cardioversion (ECV). In this study, we aimed to evaluate HRV, AFR, and SampEn in AF patients with acute ischemic stroke compared to those after stroke recovery (post-stroke) to test the hypothesis that recovery of cardiac autonomic control relates to improved degree of AF signal irregularity. Methods: Patients (age 40-80 years) with AF and acute ischemic stroke (n=12) or post-stroke (n=6) were recruited. The ECG recordings (Power Lab, fs 1000 Hz, bandwidth 20-50 Hz) were performed within 24 hours after admission or at the OPD visit, thereafter HRV, AFR, and SampEn were analyzed. Results: AFR and SampEn tended to decrease in post-stroke patients although there were no significant differences. HRV analysis showed an increase in LF/HF ratio (0.571+0.459 vs. 0.477+0.317) after stroke recovery, while both biosignals decreased in post-stroke patients compared to acute stroke group (AFR; 401+90 fpm vs. 408+74 fpm, and SampEn; 0.129+0.021 vs. 0.132+0.024). Conclusion: This preliminary study indicates that the degrees of AF signal irregularity decreaseconsistently with HRV improvement in AF patients recovered from ischemic stroke, possibly due to the interactions in brain-heart axis. • Patients (age 40-80 years) with AF and acute ischemic stroke (n=12) including those with post-stroke (n=6) were recruited. • The ECG recordings (Power Lab, sampling rate of 1000 Hz, bandwidth 20-50 Hz, 5-minute long) were performed within 24 hours after admission or at the OPD visit. • Standard short-term HRV, AFR, and SampEn were analyzed bysoftware algorithms developed in Matlab. 500 450 400 AFR (fpm) 350 300 250 Figure 4: Atrialfibrillatory rate or AFR (left) and sample entropy or SampEn (right) in post-stroke patients compared to acute stroke group. Acute stroke Post-stroke Discussion The major findings of this study indicate possible correlations between a degree of cardiac autonomic dysfunction determined by HRV parameter (LF/HF ratio) and potential biosignal markers for severity of AF (AFR and SampEn) in patients with ischemic stroke. Furthermore, previous studies have shown that the mechanisms relevant to autonomic abnormalities that precipitate AF are thought to be an increased vagal tone that causes unequal shortening of atrial refractoriness, thus creates electrophysiological heterogeneity. From these considerations, the degree of dysfunction of autonomic tone may be related to the severity of AF signal irregularity. Therefore, a decreased AF electrical complexity after stroke recovery according to an improved HRV could imply the underlying interaction in the brain-heart axis. Further studies are needed to warrant this hypothesis. Figure 1: Illustrated diagram of the ECG analysis. Background Figure 2: QRST cancellation (left) and atrialfibrillatory frequency with atrialfibrillatory rate or AFR (right). Conclusion AF is the most common cardiac arrhythmia associated with an increased risk of ischemic stroke. In Thailand, the prevalence of AF is 5 per 100,000 populations, and the mortality risk due to systemic embolization including ischemic stroke increases to 1.5-1.9compared to healthy populations in the same age group. In the other way around, approximately 15-21%of stroke patients have AF. This reflects that ischemic brain injury also affects autonomic control loops on the heart with particular relevance to arrhythmogenesis. Therefore, the insights in these brain-heart interactions may play a major role in treatment and prevention of AF with ischemic stroke. It has been known that HRV analysis determines cardiac autonomic function. The reduced HRV was found in acute ischemic stroke as well as chronic AF, whereas increased HRV spectral parameter (LF/HF ratio) correlated to early recurrence of AF after ECV. Moreover, the application of surface ECG signal processing techniques such as AFR and SampEn, representing the degrees of AF signal irregularity, has currently provided new determinants for AF treatment in many studies, for example, the use of these parameters for predicting AF recurrence after ECV as well as prediction of the behavior ofparoxysmal AF or PAF. Statistical analysis Values are expressed as mean + SD. Comparisons of data among different groups were performed using Student’s t-test. P < 0.05 was considered statistically significant. The degrees of AF signal irregularity tend to decrease consistently with HRV improvement in AF patients recovered from ischemic stroke, possibly due to the interactions in brain-heart axis. Results References/Acknowledgement 1) There were no significant differences in any clinical patient characteristics between acute stroke and post-stroke group. 2) In spite of no significant difference, HRV analysis showed an increase in LF/HF ratio (0.571+0.459 vs. 0.477+0.317) after stroke recovery (Figure 3), while AFR and SampEn decreased in post-stroke patients compared with acute stroke group (401+90 fpm vs. 408+74 fpm and 0.129+0.021 vs. 0.132+0.024, respectively) (Figure 4). • Sinnreich R, Kark JD, Friedlander Y, Sapoznikov D, Luria MH. Five minute recordings of heart rate variability for population studies: repeatability and age-sex characteristics. Heart. 1998;80(2):156-62. • Bollmann A, Husser D, Mainardi L, Lombardi F, Langley P, Murray A, et al. Analysis of surface electrocardiograms in atrial fibrillation: techniques, research, and clinical applications. Europace. 2006;8(11):911-26. • Alcaraz R, Rieta JJ. A review on sample entropy applications for the non-invasive analysis of atrial fibrillation electrocardiograms. Biomedical Signal Processing and Control. 2010;5(1):1-14. • Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillation: a translational appraisal. Physiological Reviews. 2011;91(1):265-325. • This study is supported by the National Research University Project of Thailand Office of Higher Education Commission, Thammasat university ( 2011-2013). Hypothesis In this study, we aimed to evaluate HRV, AFR, and SampEn in AF patients with acute ischemic stroke compared to those after stroke recovery (post-stroke) to test the hypothesis that recovery of cardiac autonomic control relates to improved degree of AF signal irregularity. Figure 3: Low-frequency/high-frequency power (LF/HF) ratio in post-stroke patients compared to acute stroke group.