Download
1 / 7
70 likes | 906 Views
DISODERS OF THYROID GLAND. Ass.prof. of hospital pediatrics department. HYPOTHYROIDISM

E N D
DISODERS OF THYROID GLAND Ass.prof. of hospital pediatrics department
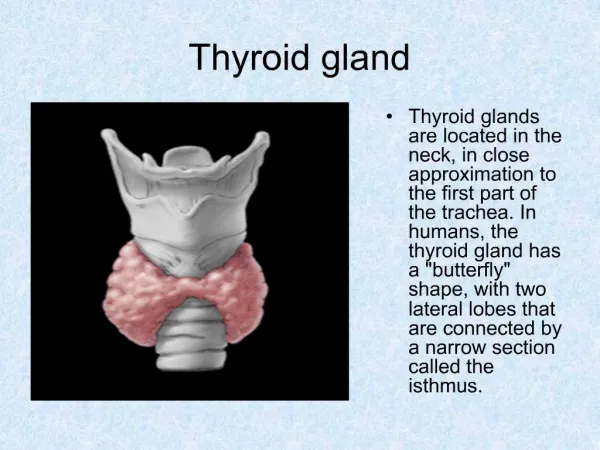
HYPOTHYROIDISM Hypothyroidism results from deficient production of thyroid hormone or a defect in its receptor. The disorder may be manifest from birth. When symptoms appear after a period of apparently normal thyroid function, the disorder may be truly "acquired" or may only appear so as a result of one of a variety of congenital defects in which the manifestation of the deficiency is delayed. The term cretinism is often used synonymously with congenital hypothyroidism but should be avoided
CONGENITAL HYPOTHYROIDISM Congenital causes of hypothyroidism may be sporadic or familial, goitrous or nongoitrous. In many cases, the deficiency of thyroid hormone is severe, and symptoms develop in the early weeks of life. In others, lesser degrees of deficiency occur, and manifestations may be delayed for months or years.
TREATMENT. Sodium-L-thyroxine given orally is the treatment of choice. Because 80% of circulating T3 is formed by monodeiodination of T4, serum levels of T4 and T3 in treated infants return to normal. This is also true in the brain, where 80% of required T3 is produced locally from T4. In neonates, the dose is 10–15 m{mu}g/kg (37.5 or 50 m{mu}g/24 hr). Levels of T4 and TSH should be monitored and maintained in the normal range. Children with hypothyroidism require about 4 m{mu}g/kg/24 hr, and adults require only 2 m{mu}g/kg/24 hr. Later, confirmation of the diagnosis may be necessary for some infants to rule out the possibility of transient hypothyroidism. This is unnecessary in infants with proven thyroid ectopia or in those who manifest elevated levels of TSH after 6–12 mo of therapy owing to poor compliance or an inadequate dose of T4. Discontinuation of therapy at about 3 yr of age for 3–4 wk results in a marked increase in TSH levels in children with permanent hypothyroidism. The only untoward effects of sodium-L-thyroxine are related to its dose. An occasional older child (8–13 yr) with acquired hypothyroidism may develop pseudotumor cerebri within the first 4 mo of treatment. In older children, after catch-up growth is complete, the growth rate provides an excellent index of the adequacy of therapy. Parents should be forewarned about changes in behavior and activity expected with therapy, and special attention must be given to any developmental or neurologic deficits.
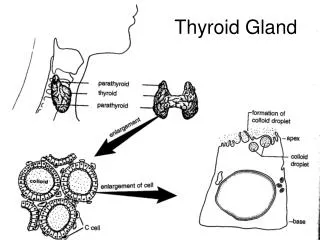
THYROIDITIS LYMPHOCYTIC THYROIDITIS (Hashimoto Thyroiditis; Autoimmune Thyroiditis) Lymphocytic thyroiditis is the most common cause of thyroid disease in children and adolescents and accounts for many of the enlarged thyroids formerly designated "adolescent" or "simple" goiter. It is also the most common cause of acquired hypothyroidism, with or without goiter. Its incidence may be as high as 1% among school children. ETIOLOGY. This is a typical organ-specific autoimmune disease. The condition is characterized histologically by lymphocytic infiltration of the thyroid. Early in the course of the disease, there may be only hyperplasia; this is followed by infiltration of lymphocytes and plasma cells between the follicles and by atrophy of the follicles. Lymphoid follicle formation with germinal centers is almost always present; the degree of atrophy and of fibrosis of the follicles varies from mild to moderate.
Familial clusters of lymphocytic thyroiditis are common; the incidence in siblings or parents of affected children may be as high as 25%. Autoantibodies to thyroglobulin (Tg) and human thyroid peroxidase (hTPO) in these families appear to be inherited in an autosomal dominant fashion, with reduced penetrance in males. The concurrence within families of patients with lymphocytic thyroiditis, "idiopathic" hypothyroidism, and Graves disease provides cogent evidence for a basic relationship among these three conditions. The disorder has been associated with many of the other autoimmune disorders more often than would be expected by chance alone. Autoimmune thyroiditis occurs in 10% of patients with type I polyglandular autoimmune syndrome, which consists of hypoparathyroidism, Addison disease, and mucocutaneous candidiasis. The association of Addison disease with insulin-dependent diabetes mellitus or autoimmune thyroid disease or both is known as Schmidt syndrome or type II polyglandular autoimmune disease.
Autoimmune thyroid disease also tends to be associated with pernicious anemia, vitiligo, or alopecia. TPOAb are found in approximately 20% of white and 4% of black children with diabetes mellitus. Autoimmune thyroid disease has an increased incidence in children with congenital rubella. Lymphocytic thyroiditis is also associated with certain chromosomal aberrations, particularly Turner syndrome and Down syndrome. The pathogenetic mechanisms for these associations are not known.