Download
1 / 38
400 likes | 748 Views
Hand-Off Communications from the Emergency Department. Robin Gordon, Paris Community Hospital Paris, IL. Review of Regulatory Standards. EMTALA Joint Commission National Patient Safety Goals. EMTALA Part of COBRA.

E N D
Hand-Off Communications from the Emergency Department Robin Gordon, Paris Community Hospital Paris, IL
Review of Regulatory Standards • EMTALA • Joint Commission National Patient Safety Goals
EMTALAPart of COBRA Designed to prevent hospitals from refusing to treat emergency patients or transferring them to charity hospitals or county hospitals because they are unable to pay or are covered by Medicaid.
Conditions Covered by EMTALA • Danger to patient health, function, organ or body • Acute undiagnosed pain • Pregnancy with contractions present • Psychiatric disturbances • Symptoms of substance abuse
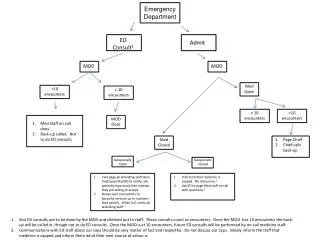
REMEMBER! If the hospital does not have the capacity, capability, or resources to provide stabilizing treatment for an emergency, an appropriate transfer must be arranged for the patient to a facility with the capacity, capability, and resources to provide the stabilizing treatment.
What is an Appropriate Transfer? • The Transferring Hospital has provided treatment to the individual with an emergency medical condition within capacity of the hospital • The Transferring Hospital has obtained agreement to accept the patient from the Receiving Hospital, including identifying a Physician to accept the patient
What is an Appropriate Transfer?(continued) • The Transferring Hospital has provided sufficient data, including medical records, X-Rays, lab reports as available, to the Receiving Hospital to facilitate continuing evaluation and treatment • The Transferring Physician has certified the transfer and arranged for the use of appropriate mode of transportation, personnel, and equipment
Joint CommissionNational Patient Safety Goal #2 Improve the effectiveness of communication among caregivers 2C – Measure, assess, and if appropriate, take action to improve the timeliness of reporting, and the timeliness of receipt by the responsible licensed caregiver, of critical tests and critical results and values.
Joint CommissionNational Patient Safety Goal #2 Improve the effectiveness of communication among caregivers 2E – Implement a standardized approach to “hand-off” communications, including an opportunity to ask and respond to questions.
Joint CommissionNational Patient Safety Goal #2 Improve the effectiveness of communication among caregivers 2E – Implement a standardized approach to “hand-off” communications, including an opportunity to ask and respond to questions.
The primary objective of a “hand-off” is to provide accurate information about a patient’s care, treatment, services, current condition, and any recent or anticipated changes.
Implementation Expectations • Interactive – allowing for the opportunity for questioning • Up-to-date information • Verification of information received • Opportunity for receiver to review relevant information • Minimizing interruptions during hand-offs
Important Information to “Hand Off” • Presenting Problem • Current Situation • Verification of Understanding
Problem with effective communication • Missing patient information from shift to shift • Missing patient information from department to department • Not everyone thinks of all of the same information when giving report. ER will give you what is important to them but other nurses often think along different lines.
What are your needs? • Each facility needs to research what their specific informational needs are and can adjust the SBAR to fit those needs. • We started out with the basic SBAR and informal training.
Informal training • Printing 3x5 note cards for the nurses to carry in their pockets • Printing large examples and placing at the nurse’s station and in the report room • Talking with staff at departmental meeting and in flyers of what the SBAR and need for the nurses to use the tool for each report
SBAR: fitting your needs • The SBAR has broken down the pertinent information into four areas: • Situation • Background • Assessment • Recommendations
Situation • Patient name • Room number • Admission date • Physician(s)
Background • Co-morbidities • Allergies • Code status • Current vitals • Recent medication given/blood thinners • Abnormal or pertinent labs/diagnostics • Special communication needs • Significant psychosocial issues
Background (cont.) • LOC • Oxygenation • Tubes/lines/drains/isolation
Assessment • Review of orders • Readiness for surgery/procedure • Mobility or safety issues
Recommendations • Goal of treatment • Reason for transfer • Anything left to do?
Audit • Informal audit • Come into report and see what was being said • Would have cards at the side but still went off the kardex often forgetting valuable information • Critical Care went off of their report sheets • We needed something different
What was wrong? • Nurses did not feel as if the information flowed • Nurses did not have a clear understanding of what was expected • “I’ve been giving report for ____ years” “I know what I’m doing”
Revamping SBAR • Looked at how to change SBAR to better fit our needs • Used the same basic format just changed the background and assessment • Again we used the 3x5 note card for visual reminders • Also took a more formal approach with the education process
The new SBARSituation • Patient name • Room number • Admission date • Managing MD • Code status • Diagnosis • Age • Brief statement or concerns
Background • Co-Morbidities (medical history) • Allergies • Recent medications given/blood thinners • Abnormal or pertinent labs/diagnostics • Special communication needs • Significant psychosocial issues • Procedures done in last 24 hours and outcomes • Safety issues
Assessment • Biophysical assessment (abnormals) • Vital signs • Implantable devices • Dressing changes • NG/Drain output • IV fluids/drips/site; when is site to be changed • Current pain score-what has been done to manage pain • Rhythm (if on telemetry) • Review of orders
Recommendations • Do we need a change in the plan? • What are you concerned about? • What are your comfortable with? • Discharge planning • Pending labs/x-rays, ect. • We need to request a change in _______(diet, activity, medication) • We need to request a consult with PT/OT/ST, dietician, diabetes educator
Formal education • Held workshops for staff members • Small groups • Visual and verbal presentations of present way and SBAR way to give report • Staff shown how important information could be missed and by having a consistent manner in which to give report the receiving nurse would know if something is missing • Each staff member would give report to another using the SBAR format with the guidance of an instructor. • Each staff member was required to competency with the SBAR approach
Audit • Audit sheets were made to encompass the SBAR report process (See example in packet) • Coordinators and House Supervisors audited: • Shift report • Intradepartmental transfers • Transfers to other facilities
How was it going? • Noted some improvement but still work needed • Nurses still were reading off of the kardex instead of giving a true handoff report • Interdepartmental transfers still needed work
Start the process again • After reviewing the process it was decided the kardex needed to be changed to a SBAR format • Again in this process we are coming up with one for the hospital as a whole but using a weekly audit to fit the needs of the patient information • To change critical care report sheet
After the kardex change • Audits reveal better reporting • Still need for improvement • Will use one on one approaches with the nurses regarding their effort in embracing the SBAR format • Will continue the Audits
Our Goal • To implement a Rapid Response Team • Need Nurse to MD SBAR • Requires having understanding and being able to effectively use the SBAR