Download

1 / 12
120 likes | 269 Views
A new pathway for the regulation and governance of health research . Professor Deborah Ashby Co-Director of Imperial Clinical Trials Unit School of Public Health Imperial College London. Reviewing the regulation and governance of health research.

E N D
A new pathway for the regulation and governance of health research Professor Deborah Ashby Co-Director of Imperial Clinical Trials Unit School of Public Health Imperial College London
Reviewing the regulation and governance of health research • Building on UK strengths and recent investment. • Government commission – project launched March 2010 • Reported January 2011 Scope: • ‘Health research’. • Review the landscape and make recommendations to increase the speed of decision-making, reduce complexity and eliminate unnecessary bureaucracy and cost. Process: • Academy working group. • Two calls for evidence – over 300 submissions.
Key bottlenecks (1) Delays and duplication in obtaining research permission from NHS R&D Trusts. Replication of study-wide checks by each individual Trust. Inconsistency in the interpretation of checks, such as requirements to access patient data. Overlap in checks by NHS Trusts with responsibilities of NRES or MHRA. Lack of oversight of the NHS permission process for multi-site studies Complexity and inconsistency across the regulatory pathway e.g. access to patient data. Regulation and governance pathway developed in a piecemeal manner. Multiple approval bodies and layers of checks, leading to conflicting advice and variable standards. Checks often undertaken in series rather than parallel.
Key bottlenecks (2) A lack of proportionality in the regulation of clinical trials. A ‘one-size’ fits all interpretation of the European Clinical Trials Directive. Experimental medicine studies being inappropriately classified within the scope of the Directive. Increased administrative burden and cost of trials. A healthcare culture that fails to fully support the value and benefits of health research. Much excellent research, but generally given a low priority. Opportunity to enhance the culture of research as part of changes to the structure of the NHS. Challenges around excess treatment costs. Situation is stifling research Cancer Research UK: An average of 621 days from confirming funding to recruitment of the first patient.
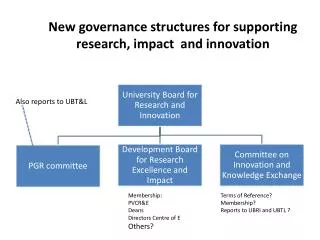
Main recommendations (1) Establish a new single research regulator to rationalise the regulation and governance of all health research. To oversee and manage a single coordinated pathway. Remove unnecessary complexity and become a ‘one-stop’ shop for research regulation. Facilitate a proportionate approach that allows researchers and regulators to focus on the specific benefits and risks of a given study. Introduce a streamlined, consistent process for NHS R&D permissions The creation of a new National Research Governance Service (within the new regulator) to undertake all study-wide checks to national standards. Introduce new timelines for NHS R&D permission, with future NIHR funding linked to performance.
Main recommendations (2) Streamlining access to patient data while maintaining appropriate safeguards. Remove the approval of research studies from the remit of Caldicott Guardians. A need for mechanisms that allow approved members of research teams to identify eligible patients for research studies. Revision of the European Clinical Trials Directive and a more proportionate approach by the MHRA to clinical trials regulation and monitoring. Ensure that approval and monitoring requirements are proportionate to risk. Reduce the scope of the Directive. Simplify the requirements for safety reporting. Health research formally and irreversibly embedded into NHS leadership and governance processes. Key metrics and indicators of research activity published by all Trusts. Provision of co-ordinated information for patients and the public about the role and benefits of health research.
Support from across the community. Andrew Lansley MP, Secretary of State for Health said: “National regulation and local governance of health research are too complex and scattered across too many different bodies. The Academy's report makes the case for simplification under a health research agency that will streamline and co-ordinate regulatory and governance processes”. Sir Mark Walport, Director of the Wellcome Trust, said: "This report and its recommendations are both welcome and timely..… We must strike a better balance between protecting participants involved in research and not unduly or inappropriately obstructing the progress of research that will bring important health benefits.“ Harpal Kumar, chief executive of Cancer Research UK, said “We strongly welcome the report and support its recommendations. We believe that a single health research agency could reduce the time it takes our researchers to get approval for their studies to 60 days – around a fifth of the time it takes them now.”
The Government’s response (March 2011) ‘In life sciences…we will radically reduce the time it takes to get approval for the clinical trials.’ George Osborne • Focus on ‘healthcare and life sciences’ as a key sector for long-term growth. • Commitment to take forward many of AMS key recommendations.
The Plan for Growth (1) “Set up a new health research regulatory agency (HRRA) this year to combine and streamline approvals for health research” (Plan for Growth). To be established as Special Health Authority by December 2011. Legislation laid before Parliament October 2011 (last week). In the first instance, this is likely to consist solely of the National Research Ethics Service (NRES). “Link NHS research funding to hospital performance on R&D approval and patient recruitment” (Plan for Growth) Future NIHR funding will become conditional on Trusts adopting new Research Support Services: a ‘bottom-up’ approach to standardising good practice. Funding conditional on meeting benchmarks in the R&D approval process. Trusts will publish metrics on their performance.
The Plan for Growth (2) “The Government will reduce perceived gold-plating and increase the proportionality of the EU Clinical Trials Direcetve and its application” (Plan for Growth). “Government will seek to influence the Commission to bring forward soundly based proposals to reduce regulatory burdens in the European Clinical Trials Directive”. “The Government will look to introduce a number of domestic measures that would achieve some of the AMS’s aims but in a shorter timeframe than is possible through the EU”
What is needed now? • The Government have begun to implement a number of the Academy’s recommendations. • There now needs to be a clear and comprehensive vision of: • the future functions of the HRA; • a timetable for its creation; • and clarity on how it will deliver coordination and oversight across a single regulatory and governance pathway. • Agreement on the role and responsibilities of different stakeholders in monitoring and supporting the successful implementation of the recommendations.