Download
1 / 26
310 likes | 629 Views
What is an imprinted gene? Using Prader-Willi and Angelman syndrome as an example describe the imprinting control centre and explain how the imprint is maintained or erased within the germline. What are the clinical and diagnostic implications of errors in this process.

E N D
What is an imprinted gene?Using Prader-Willi and Angelman syndrome as an example describe the imprinting control centre and explain how the imprint is maintained or erased within the germline. What are the clinical and diagnostic implications of errors in this process
What is an imprinted gene? • Definition of imprinting: “monoallelic expression of biallelic genes according to parent of origin” • According to mendelian inheritance, autosomal genes are expressed from both maternal and paternal alleles (functionally equivalent), resulting in biparental expression. • Imprinted genes however are only expressed from one chromosome in a parent of origin specific manner. • The allele that is inactivated is termed imprinted. • There is no change in nucleotide sequence of any of the genes involved. This is called an epigenetic mutation.
Characteristics of imprinted regions • Imprinted genes show several typical features: • Monoallelic expression • Differential DNA methylation (Razin et al, 1994) • Asynchronous DNA replication of the maternal and paternal alleles (Knoll et al, 1994, Kitsberg, 1993) • Imprinted regions often have several of the following unusual features in common: • There is a complex array of genes, sometimes overlapping within the cluster • Genes within the cluster may have different parental imprints • All genes within cluster are frequently regulated in a co-ordinated way • Differential DNA methylation • Anti-sense transcripts and non-coding RNA is involved • The imprinting process appears to be mediated by imprinting centres located within each imprinted region.
Mechanisms • The exact mechanisms still being deciphered, however recognised to be multi-step process involving: • Imprinted genes must be marked differently in the male and female germlines • Imprint must be stably maintained in soma as cells divide and differentiate • Must be recognised by cells transcriptional machinery to produce monoallelic expression • Finally, imprint must be erased and reset in the germ cells Failure at any of these steps will result in a loss of imprinting • 3 possible imprint marks have been proposed: • DNA methylation • Alterations to chromatin structure • Asynchronous replication timing
Prader Willi Syndrome & Angelman Syndrome • Clinically distinct neurobehavioral genetic disorders that map to an imprinted region on 15q11-q13.
15q11-q13 • 2Mb imprinted cluster contains numerous genes and RNA transcripts that apparently lack protein-coding potential: • majority maternally imprinted (paternal only expression) • UBE3A & ATP10C exhibits maternal specific expression during early brain development. • Some not imprinted • PWS believed to be contiguous gene syndrome, in which loss of expression of several genes is required for full manifestation of the disorder • AS believed to arise through loss of expression from a singlematernally expressed gene, UBE3A
Imprinting mutations • Show typical methylation pattern associated with either PWS or AS but biparental inheritance. • AS patients with imprinting mutations have paternal methylation pattern only (Maternal chromosome carries paternal imprint) • PWS patients with imprinting mutations have maternal methylation only (paternal chromosome carries maternal imprint) • Represents a defect in setting the imprint. In PWS, IC defects block maternal to paternal switch In AS, IC defects block paternal to maternal switch
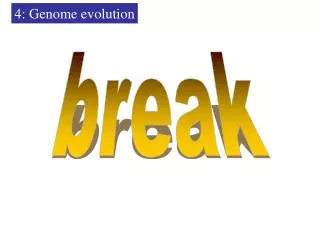
A: In somatic cells (green squares) of a male or female individual, the maternal chromosome carries a maternal imprint. It is erased in primordial germ cells (yellow cells), newly established during later stages of gametogenesis (yellow circles) and maintained in the zygote and embryo (blue squares). Imprinting errors (indicated by red arrows) can result from : B: failure in imprint erasure C: Imprint establishment D: or imprint maintenance (Imprint maintenance errors lead to somatic mosaicism)
Imprinting mutations • Possible causes: • Occur without any DNA sequence changes (primary epimutations, - Believed to arise from a developmental failure to switch) - Majority cases • Result from mutations in cis-regulatory elements or trans-acting factors (secondary epimutations) ~10%
Imprinting centre mutations have no phenotypic effect as long as the sex of the transmitting parent does not change. • PWS IC deletion has no phenotypic effect when transmitted through female germline but leads to an incorrect maternal imprint on paternal chromosome when inherited from a male • AS IC deletions have no effect when transmitted through male germline but lead to incorrect paternal imprint when transmitted through female germline
Small deletions within the IC have been identified in a proportion of both PWS and AS patients. Analysis of the shortest region of overlap (SRO) has distinguished 2 slightly different key regions. • PWS IC deletions identified SRO is 4kb spanning the first exon and promoter of the SNURF-SNRPN locus. • The SRO of deletions in AS cases has been narrowed down to 880bp, 35kb upstream of SNRF-SNRPN. (NB. Doesn’t include the UBE3A gene) • As two regions do not overlap, suggests a bipartite IC.
Mechanism in 15q11-q13 Study by Buiting et al, 1998 & 2003 • 18 AS patients with IC deletions (incorrect paternal imprint) • 11/18 inherited IC deletion from maternal grandfather • 7/18 inherited IC deletion from maternal grandmother =suggests that the imprint defect occurred after erasure of parental imprints ie, from an error in imprint establishment or maintenance • 19 PWS patients with IC deletions (incorrect maternal imprint) • 19/19 inherited IC deletion from paternal grandmother = suggests incorrect imprint results from failure of paternal germline to erase the grandmaternal imprint
Buiting et al, have proposed an imprinting model that involves a two stage imprint switch. • They hypothesis that the first stage is the erasure of the previous imprint and the second stage is the establishment of a new imprint. • PWS occurs due to an inability to erase the previous maternal imprint whereas AS occurs due to an inability to establish a new maternal imprint.
Active PWS-SRO on paternal allele ‘activates’ all paternal genes across the PWS/AS domain. • AS-SRO apparently serves as a ‘repressor’ of the PWS-SRO on the maternal allele
Diagnostic Approaches Cytogenetic Analysis Routine Karyotype • Detects translocations, inversions & other chromosome abnormalities • Disadvantages: difficult to detect interstitual deletions & cannot detect UPD FISH • Detects deletions • Disadvantages: Unable to determine parental origin of each chromosome = cannot detect UPD = if deletion identified are unable to distinguish AS from PWS
Molecular diagnosis • Parental specific expression is mediated by differences in methylation and detection of these methylation differences provides the basis for initial molecular diagnosis. • Evaluates the methylation status of the SNRPN CpG island. • PWS = loss of unmethylated paternal allele • AS = loss of methylated maternal allele • Originally carried out by Southern blot based approach. • Now normally carried out using methylation specific PCR. • The methylation test does not distinguish between a deletion and UPD – although this isn’t necessary for confirmation of clinical diagnosis. • If the resulting methylation pattern is characteristic of AS or PWS then microsatellite analysis carried out to determine whether cause is a deletion, UPD or imprinting defect.
Southern Blot Analysis using SNRPN probe KB17 Analysis involves a double restriction digest - one enzyme (XbaI) cuts both the maternal and paternal DNA - second enzyme (NotI) only cuts unmethylated paternal DNA Detects PW and AS cases which result from deletions, UPD and imprinting mutations (Sensitivity is almost 100% for PWS and ~80% for AS ) PWS patients only have a 4.2kb band (maternal methylated chromosome) AS patients only have a 0.9kb band (paternal unmethylated chromosome) PWS Normal AS Maternal chromosome Disadvantages: 1. Will miss very small deletions for AS. 2. Does not distinguish between cases of UPD and deletion (which have low recurrence risks) from imprintor mutations where the recurrence risks are 50%. Paternal chromosome
Methylation Specific PCR • Sodium bisulfite treatment of genomic DNA: • Has no effect on methylated DNA (maternal) • Converts cytosine to uracil when DNA is unmethylated (paternal) • Followed by Multiplex PCR using a common reverse primer and 2 sets of allele specific primers: • MET primers only bind to & amplify methylated DNA • UNMET primers only bind to & amplify unmethylated DNA • In PWS – only the maternal methylated allele is present = only MET primers amplify • In AS - only the paternal unmethylated allele is present = only UNMET primers amplify Normal PWS AS Maternal band Paternal band
PCR Microsatellite Analysis • Amplifies highly informative polymorphisms from the PWS/AS critical region. • Ideally requires analysis of both parents and proband • Loss of paternal contribution = confirms PWS (either a de novo deletion or maternal disomy) • Loss of maternal contribution = confirms AS (either a de novo deletion or paternal disomy) in AS. • Biparental inheritance = imprinting defect. Presence of small deletions should be rules out by extensive analysis of markers from the SRO. Cases can then be referred to research lab. • Further analysis using microsatellites distal to 15q required to distinguish between de novo deletions and uniparental disomy for genetic counselling purposes.
Recurrence Risks *In absence of any structural abnormality, <1%. For unbalanced translocation could be as high as 50%
IC mutation recurrence risk • IC deletions can occur de novo or majority are inherited. • Familial IC deletion associated with 50% recurrence risk • Primary epimutations can occur: • During imprint erasure in primordial germ cells • Imprint establishment during later stages of gametogenesis • Imprint maintenance after fertilisation = somatic mosaicism If occur after fertilisation = low risk. If father germline mosaic = upto 50%
Prenatal testing • Although methylation patterns can differ between CVS DNA and somatic tissue DNA, correct prenatal diagnoses are obtained when using the 5’SNRPN locus.
References • EMQN best practice guidelines • London IDEAS Genetics Knowledge Park Learning support for PWS & AS • Series of review on imprinting in Cytogenetic Genome Res (2006)113. Specifically: • Kantor et al, 2006. The PWS/AS imprinted domain and its control centre. Cytogenetic Genome Res 113: 300-305 • Horsthemke & Buiting, 2006. Imprinting defects on human chr 15. Cytogenetic Genome Res 113: 292-299 • Bielinska et al, 2000. De novo deletions of SNRPN exon 1 in early human and mouse embryos results in a paternal to maternal imprint switch. Nature Genetics, 25, 74-78 • Horsthemke et al, 1997. Structure and function of the chromosome 15 imprinting centre. J Cell Physiology 173:237-241