Download
1 / 66
770 likes | 1.15k Views
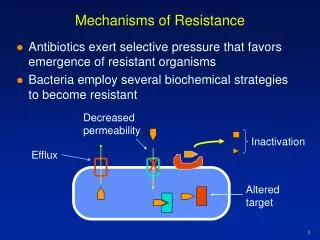
Formal evidence in patients still pending. POSSIBLE MECHANISMS OF IMATINIB RESISTANCE . BCR/ABL gene dependent Point mutations at catalytic site of BCR/ABL gene BCR/ABL gene amplification BCR/ABL gene up-regulation BCR/ABL gene independent Increase of protein binding

E N D
Formal evidence in patients still pending POSSIBLE MECHANISMS OF IMATINIB RESISTANCE • BCR/ABL gene dependent • Point mutations at catalytic site of BCR/ABL gene • BCR/ABL gene amplification • BCR/ABL gene up-regulation • BCR/ABL gene independent • Increase of protein binding • Additional genetic events • Quiescent Ph+ cells relatively insensitive to imatinib
CRYSTAL STRUCTURE OF cABLDomains of the catalytic site Nucleotide-binding loop Activation loop Catalytic loop
cAbl Irk Hck MOLECULAR MODELING OF TKS’ ACTIVATION The role of the activation loop domain: Switching from gate-closed form (inactive) to gate-open form (active)
IMATINIB-cABL INTERACTION:Stabilization of cABL inactive form Activation loop
MAP OF ABL MUTATIONS 33 32 24 20 9 6 6 6 5 4 3 2 1 1 1 1 1 1 1 1 1 catalytic domain activation loop ATP-binding loop M244V V289A L248V H396R/P M343T E255K/V G250E L387M M351T F359V S417Y Y253F/H T315I E355G/D E459K F382L Q252R/H F311L/I F317L V379I F486S Last update Feb 04
PATTERNS OF IMATINIB RESISTANCE IN Ph+ LEUKEMIAS CML clone Treatment with Imatinib Primary Resistance Cytogenetic response Reemergence of Ph chromosome Acquired (Secundary) Resistance
BCR/ABL MUTATIONS IN FRONT-LINE AND ACQUIRED RESITANCE TO IMATINIB
BCR/ABL BCR/ABL Hypothesis front-line resistance = clonal evolution Non Responder Responder Imatinib Imatinib Ph Other defects Proliferation Proliferation The resistant clone is already the main component of the Ph-positive cell population
CML/002/STI571 protocol 56/200 pts: never achieved a MCgR (28%) 40/56 pts: residual material available for mutational analysis all 40 patients analyzed in parallel by DHPLC and sequencing
CML/002/STI571: RESULTS 19/40 (45%) patients who had cytogenetic refractoriness to Imatinib showed evidence of a point mutation 8 11 catalytic domain activation loop P- loop M244V M343T 298 L248V H396R/P E255K/V L387M G250E M351T F359V S417Y Y253F/H T315I E355G/D E459K F382L Q252R/H F311L/I F317L F486S V379I
DETECTION OF ABL MUTATIONS MAY BE CLINICALLY IMPORTANT • The presence of some specific mutations may offer prognostic information • Different mutants show different degrees of resistance to Imatinib
MUTATED vs. NON-MUTATED Dead Progression to AP/BC Mutated 11/19 7/19 Non-mutated 0/22 2/22 Time to progression Overall Survival
P-LOOP vs. NO P-LOOP Progr. to AP/BC Dead P-loop 9/11 6/11 No P-loop 2/8 1/8 Overall Survival Time to progression
PROGNOSTIC SIGNIFICANCE OF P-LOOP MUTATIONS Figure 2.Kaplan-Meier survival curves for patients with mutations. There was a significant difference in the survival rate of patients in AP and late-CP with P-loop and non–P-loop mutations. With one exception, patients with P-loop mutations died. (Brandford et al, Blood 2003)
FACTORS WHO AFFECT PROBABILITY OF BCR/ABL MUTATION DETECTION (Brandford et al, Blood 2003)
CML CONCLUSIONS • Cytogenetic and Molecular response are relevant surrogate marker for CML monitoring • Resistance to STI571 is a complex phenomenon and search for point mutation is crucial for CML patient management.
SPECIFIC GENOTYPES OF ALL Adult ALL Childhood ALL T-Cell ALL
Adult Ph+ ALL: MRC UK ALL12/ECOG E2993 Study Outcomes • 1389 patients with ALL • 267 (19%) Ph+ ALL • CR 76% • 5-yr OS 23% • 5-yr EFS 18% Goldstone et al. Blood. 2003;102:80a - Abs 268
IMATINIB IN THE TREATMENT OF Ph+ ALL • Monotherapy - Salvage treatment - Maintenance therapy after chemotherapy in newly diagnosed patients - “First line” induction for newly diagnosed patients - MRD treatment after SCT • Combination treatment with: - Chemotherapy in newly diagnosed patients Hyper-CVAD JALSG ALL202 Study - IFN-a in advanced stage patients
Imatinib Monotherapy in Relapsed/Refractory Ph+ ALL Response to Treatment (Imatinib 400 or 600 mg/d) Ph+ ALL CML LyBC n = 48 n = 8 Hematologic response 29 (60%) 4 (50%) CR 9 (19%) 4 (50%) CR–marrow 5 (10%) 0 PR 15 (31%) 0 Failure 12 (25%) 4 (50%) Not evaluable 7 (15%) 0 Ottmann OG, et al. Blood. 2002;100:1965-1971.
Imatinib Monotherapy in Relapsed/Refractory Ph+ ALL Time to Progression 100 90 80 70 60 50 % of Patients Without Progression 40 30 Ph+ ALL (n = 48) 20 10 = Censored observations 0 0 1 2 3 4 5 6 7 8 9 10 11 12 Months Since Start of Treatment Ottmann OG, et al. Blood. 2002;100:1965-1971.
Imatinib Monotherapy in Relapsed/Refractory Ph+ ALL Nonhematologic Drug-Related Adverse Events Ottmann OG, et al. Blood. 2002;100:1965-1971.
Imatinib Monotherapy in Relapsed/Refractory Ph+ ALL Hematologic Toxicity and Laboratory Abnormalities All enrolled patients (n = 56) Grade 3 17 (30%) 12 (21%) 15 (27%) 1 (2%) 2 (4%) 2 (4%) Grade 4 4 (7%) 15 (27%) 23 (41%) 0 0 0 Anemia Thrombocytopenia Leukocytopenia Increased ALP Increased ALT Increased bilirubin Ottmann OG, et al. Blood. 2002;100:1965-1971.
Imatinib Monotherapy in Relapsed/Refractory Ph+ ALL (studies 109/114) Relapse After Allogeneic SCT Ottmann OG, et al. Blood. 2001;98:589a-590a. Ottmann OG, et al. Ann Hematol. 2002;81(suppl 2):S36-S37 Ottmann OG, Wassmann B. Best Pract Res Clin Hematol. 2003;15:757-769 Wassmann B, et al. Blood. 2004;103:1495-1498.
Imatinib Monotherapy in Relapsed/Refractory Ph+ ALL (studies 109/114) Relapse After Allogeneic SCT
SCT 10 Imatinib 600mg/d 1 Relapse 0.1 0.01 P190/ Gus copies CHT 0.001 Vincristine + Prednisone 0.0001 Imatinib 0.00001 0.000001 Sep-99 Mar-00 Jun-00 Oct-00 May-01 Nov-01 Apr-02 Dec-02 Aug-04 PB blasts (x109/L) 39,2 0 1,0 0 0 0 0 0 0 BM blasts (%) 95 <5 30 <5 <5 <5 35 <5 <5 Donor (XY) 20/20 20/20 20/20 25/30 19/20 25/26 mitosis Ph+ mitosis 15/15 - 12/20 0/20 0/20 0/20 5/30 0/20 0/26
Imatinib Monotherapy in Relapsed/RefractoryPh+ ALL: Phase II Studies 109/114 Salvage before allogeneic SCT 46 Ph+ ALL patients with relapsed or refractory disease enrolled 16 patients ineligible for SCT (age, comorbidity, or patient refusal)30 patients eligible for SCT 18 patients treated with imatinib for refractory disease 12 patients treated with imatinib for relapsed disease 22 patients transplanted at a median of 67 days (range, 34–246 days) after starting imatinib Wassmann B, et al. Leukemia. 2002;16:2358-2365.
Imatinib Monotherapy in Relapsed/Refractory Ph+ ALL Considerations • Imatinib produced pronounced, albeit brief, hematologic responses in a majority of relapsed/refractory Ph+ ALL patients, including those who relapse after allogeneic SCT • Imatinib is also effective in enabling ~70% of relapsed/refractory Ph+ ALL patients to undergo subsequent allogeneic SCT • Imatinib used as salvage treatment shows a very favorable safety profile • Imatinib may also be useful in palliative treatment of patients who are not candidates for aggressive salvage therapy
Time progression 1 2 3 4 5 N N N N N Ph+ N N N N N N N N N N N N Ph+ Ph+ N N N N N N N N Ph+ N N N N Ph+ Ph+ Ph+ Ph+ N N N N N N N N Ph+ Ph+ N N N N N N N Ph+ Ph+ N Ph+ Ph+ N N N N Ph+ N N N Ph+ Ph+ N N N Ph+ N Ph+ N Ph+ N N Ph+ Ph+ N N Ph+ Ph1 Ph+ Ph+ N N N N Ph+ Ph+ N Ph1 Ph1 N Ph+ N Ph+ Ph1 N Ph1 Ph+ Ph1 Ph1 N Ph+ Ph1 Ph+ Ph1 Ph+ N Ph+ Ph1 Ph+ Ph1 Ph+ Ph1 Ph1 Ph+ Ph+ Ph+ Ph1 Ph+ Ph1 Additional genetic defects Ph1 Ph+ Ph+ Ph+ Ph1 Ph1 Ph+ Ph+ Ph+ Ph+ Ph+ Ph+ Ph1 Ph+ Ph+ Ph1 Sensitivity to Imatinib
GENOMIC INSTABILITY OF Ph+ CELLs • BCR/ABL protein causes ROS-oxidative DNA damage and its unfaithful repair Nowicki et al, Blood 2004 - prepub on line • BCR/ABL protein translocates to the nucleus and its nuclear activity leads to the impairment of DNA damage repair Dierov et al, Cancer Cell 2004
m-bcr ALL M-bcr ALL M-bcr CML BCR-ABL / CG NCN NS NS p=0.001 p<0.001 n = 24 17 29 24 17 29 24 17 29 ABL B2M/100 GUS BCR/ABL INTRACELLULAR CONTENT OF ACUTE AND CHRONIC Ph+ LEUKEMIAS Does the high BCR/ABL content of Ph+ acute leukemias correlate with their genomic instability?
POSSIBLE MECHANISMS OF IMATINIB RESISTANCE • BCR/ABL gene dependent • Point mutations at catalytic site of BCR/ABL gene • BCR/ABL gene amplification • BCR/ABL gene up-regulation • BCR/ABL gene independent • Increase of protein binding • Additional genetic events • Quiescent Ph+ cells
Imatinib Monotherapy as Maintenance treatment Newly diagnosed Ph+ ALL pts (≤60y) after after chemotherapy GIMEMA LAL 0201 Protocol
Imatinib Monotherapy as Maintenance TreatmentThe GIMEMA 0201-A trial
The GIMEMA 0201-A trial Interim analysis
GLIVEC 10 1 0,1 0,001 0,0001 0,00001 0,000001 6 8 10 12 16 18 20 22 2 4 26 28 14 24 0 months MRD monitoring in 0201 - A trial MRD Level
GLIVEC relapse relapse relapse 10 DLI 1 0,1 DLI Allo SCT 0,001 0,0001 0,00001 6 8 10 12 16 18 20 22 2 4 26 28 14 24 0 0,000001 months MRD monitoring in 0201 - A trial MRD Level
Relapse probability according to MRD stratification after consolidation (Ph+ ALL expressing P190) 100 80 60 40 p = .03 20 0 0 4 8 12 16 20 24 *Abl mutation detected in 1 patient Relapse rate (%) (months)
Imatinib Monotherapy as Maintenance Treatment Considerations • Imatinib given as single agent is an highly effective post-consolidation therapy • In patients with P190BCR/ABL gene unsatisfactory molecular response rate to conventional CHT is a powerful predictor of subsequent resistance
MRD-Triggered Imatinib After SCT Study Design CR and MRD+ Chemo- therapy Imatinib SCT CR Wassmann B, et al. EHA 2004. Abstract 612.
MRD-Triggered Imatinib After SCT Patient Features Patients 27 Male /female 14/13 Age (y) 48 (16–63) Allogeneic/autologous SCT 24/3 Graft-vs-host disease at entry 11 Months from SCT to BCR-ABL detection 3.6 (0.5–18) Months from SCT to start of imatinib 4.4 (1–19) Wassmann B, et al. EHA 2004. Abstract 612.
MRD-Triggered Imatinib After SCT Interim Results (Median follow-up of 15.6 months) Wassmann B, et al. EHA 2004. Abstract 612
MRD-Triggered Imatinib After SCT • Molecular response to imatinib therapy in Ph+ ALL patients with MRD after SCT discriminates between those likely to relapse and those likely to have sustained molecular remissions • Early assessment of BCR-ABLtranscripts in this setting may identify a subset of patients requiring treatment in addition to or other than imatinib Wassmann B, et al. EHA 2004. Abstract 612.