Download
1 / 27
290 likes | 612 Views
ALLHAT. ATRIAL FIBRILLATION AT BASELINE AND DURING FOLLOW-UP in The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial November 9, 2003. L. Julian Haywood, Charles E. Ford , Richard S. Crow, Barry R. Davis, Paula T. Einhorn, Angela Williard, and Barry Massie. ALLHAT.

E N D
ALLHAT ATRIAL FIBRILLATION AT BASELINEAND DURING FOLLOW-UPinThe Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack TrialNovember 9, 2003 L. Julian Haywood, Charles E. Ford, Richard S. Crow, Barry R. Davis, Paula T. Einhorn, Angela Williard, and Barry Massie
ALLHAT Purpose • To document the prevalence of atrial fibrillation (AF) or atrial flutter (AFL) at baseline and its new appearance during follow-up in ALLHAT. • To determine the influence of AF/AFL at baseline on outcome in ALLHAT.
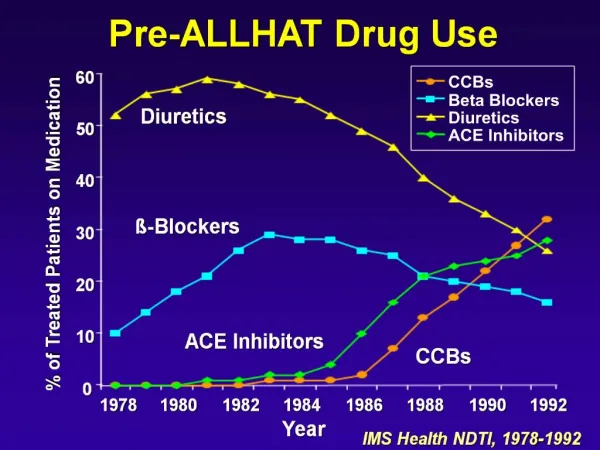
ALLHAT Background • Randomized, double-blind, multicenter trial • Determined whether fatal CHD or nonfatal MI was lower for high-risk hypertensives treated with amlodipine (CCB), lisinopril (ACEI), doxazosin (alpha blocker) vs chlorthalidone (diuretic) • Atrial fibrillation (AF) is the most common serious arrhythmia affecting morbidity and mortality.
ALLHAT Methods • Standard 12-lead ECGs, recorded at baseline and at 2-year intervals during follow-up, were coded for Q-wave abnormalities, ST-segment depression, T-wave inversion, LVH, bundle branch block, and atrial fibrillation or flutter, using the Minnesota Code. • Univariate and multivariate statistical methods were used to determine prevalence, incidence, and prognosis as relates to multiple clinical parameters, and according to treatment group.
ALLHAT Sample Size and Number (%) of Participants with AF • Missing a baseline ECG, but with one or more follow-up ECGs on file. • Sample size less those with no ECGs and no baseline ECG.
ALLHAT Sample Size and Number (%) of Participants with AF,Excluding Doxazosin Group • The doxazosin arm of ALLHAT was stopped in January 2000 due to higher CV events and • virtually no chance to show a difference in CHD. • b. Missing baseline ECG but one or more follow-up ECGs on file. • c. Atrial fibrillation and flutter, combined.
ALLHAT Baseline Characteristics Stratified By Atrial Fibrillation Status * Indicates statistical significance of difference (p < 0.05). ** Indicates statistical significance of difference (p < 0.01).
ALLHAT Baseline Characteristics Stratified By Atrial Fibrillation Status * Indicates statistical significance of difference (p < 0.05). ** Indicates statistical significance of difference (p < 0.01).
ALLHAT Prevalence of Atrial Fibrillation Per 1000 Participants, by Randomized Treatment Group AF prevalence was 10.9 per 1000, overall (334/30,704). Events per 1000 * Compared with chlorthalidone, neither the amlodipine nor lisinopril group differed significantly.
ALLHAT Prevalence of Atrial Fibrillation Per 1000 Participants, by Baseline Characteristics Events per 1000 Age at Entry, years * Subgroup differs significantly from comparison group (55-69, women, black) before and after adjusting for age, race, and sex (p < 0.01).
ALLHAT Prevalence of Atrial Fibrillation Per 1000 Participants, by Baseline Characteristics Events per 1000 * ASCVD subgroup differs significantly from comparison group (no ASCVD) before and after adjusting for age, race, and sex (p < 0.01).
ALLHAT Prevalence of Atrial Fibrillation Per 1000 Participants, by Baseline Characteristics Events per 1000 Subgroups do not differ significantly from comparison groups after adjustment for age, race, and sex differences.
ALLHAT Occurrence of New Atrial Fibrillation
ALLHAT Occurrence of Atrial Fibrillation Per 1000 Participants, by Randomized Treatment Group AF incidence was 17.2 per 1000, overall (551/32,042). Events per 1000 * Compared with chlorthalidone, neither the amlodipine nor lisinopril group differed significantly.
ALLHAT Occurrence of Atrial Fibrillation Per 1000 Participants, by Baseline Characteristics Events per 1000 Age, years
ALLHAT Occurrence of Atrial Fibrillation Per 1000 Participants, by Baseline Characteristics Events per 1000 Left Ventricular Hypertrophy by ECG.
ALLHAT Occurrence of Atrial Fibrillation Per 1000 Participants, by Baseline Characteristics Events per 1000 BMI = Body Mass Index Serum potassium at 3-month visit.
ALLHAT Cumulative Event Rates for All-Cause Mortality by Entry AF Status 0.40 0.35 0.30 0.25 AF Present 0.20 Cumulative Event Rate 0.15 0.10 AF Absent 0.05 0.00 0 1 2 3 4 5 6 Years to Death
ALLHAT Cumulative Event Rates for Fatal CHD or Nonfatal MI, by Entry AF Status 0.20 0.15 AF Present 0.10 Cumulative Event Rate AF Absent 0.05 0.00 0 1 2 3 4 5 6 Years to Fatal CHD or Nonfatal MI
ALLHAT Cumulative Event Rates for Stroke by Entry AF Status 0.20 0.17 0.15 AF Present 0.13 0.10 Cumulative Event Rate AF Absent 0.07 0.05 0.03 0.00 0 1 2 3 4 5 6 Years to Stroke
ALLHAT Cumulative Event Rates for All-Cause Mortality in Those with AF at Entry, by Treatment Group 0.40 0.35 0.30 0.25 0.20 Cumulative Event Rate Chlorthalidone 0.15 Amlodipine 0.10 Lisinopril 0.05 0.00 0 1 2 3 4 5 6 Years to Death
ALLHAT Cumulative Event Rates for Fatal CHD or Nonfatal MI in Those with AF, by Treatment Group 0.20 0.15 0.10 Cumulative Event Rate Chlorthalidone Amlodipine 0.05 Lisinopril 0.00 0 1 2 3 4 5 6 Years to Fatal CHD or Nonfatal MI
ALLHAT Cumulative Event Rates for Stroke by Treatment Group In Participants with AF at Baseline 0.30 0.25 0.20 0.15 Cumulative Event Rate 0.10 Chlorthalidone Amlodipine 0.05 Lisinopril 0.00 0 1 2 3 4 5 6 Years to Stroke
ALLHAT Conclusion-1 In high-risk hypertensive patients : • Prevalence of AF in ALLHAT at baseline was increased by: age, non-Black status, male gender, and presence of ASCVD. • AF at baseline was associated during follow-up with: increased overall mortality increased fatal CHD and MI increased stroke
ALLHAT Conclusion-2 • Likelihood of new onset of AF during follow-up was increased by: Age, male gender, non-Black race, CHD, ASCVD, LVH • Randomization to chlorthalidone, amlodipine and lisinopril did not influence prevalence of AF at baseline or its new appearance during follow-up. • Among participants with AF/AFL at baseline, there were no differences among randomized groups for mortality, major CHD events, or stroke.