Download
1 / 30
300 likes | 571 Views
Permanent Dentition. 1 year. The formation of the permanent dentition has been described by Schour and MassIer (1940) as occurring in clusters.

E N D
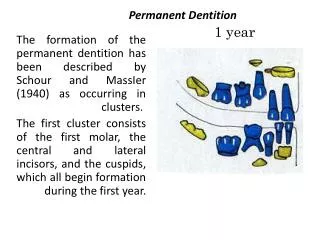
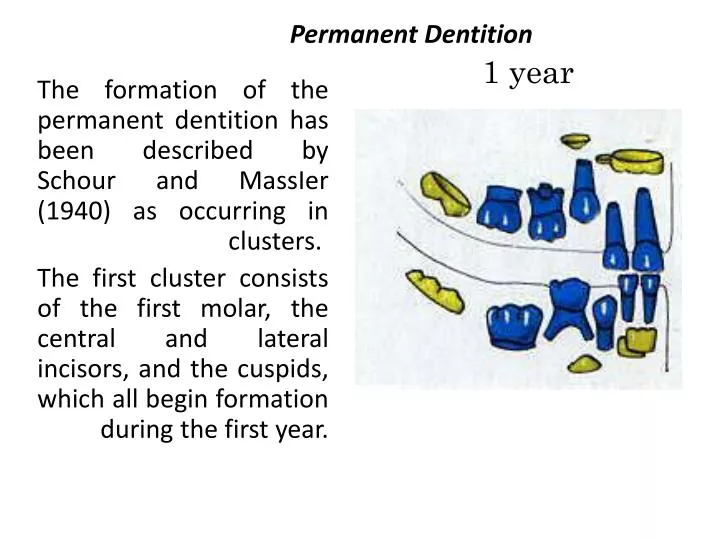
Permanent Dentition 1 year The formation of the permanent dentition has been described by Schour and MassIer (1940) as occurring in clusters. The first cluster consists of the first molar, the central and lateral incisors, and the cuspids, which all begin formation during the first year.
3 years The second cluster forms during the ages of 2-4 years. (it consists of the premolars and the second molars)
7 years The third cluster consists of the third molar, which forms some 5-6 years after the second molar, though its formation varies widely for various population groups.
5 years The first teeth of permanent dentition to emerge through the gingiva are the first molars. These teeth emerge distal to the primary second molar and are larger than any of the primary teeth.
6 years Because eruption occurs at approximately 6 years of age the teeth are often called "6-year molars." They begin to calcify at about the time of birth.
The central incisor is the second permanent tooth to emerge into the oral cavity, Eruption time occurs quite close to that of the first molar: i.e., tooth emergence occurs between 6 and 7 years. As with the first molar at 6 years 50 percent of the individuals have reached the stage considered to be the age of attainment of the stage or more specifically, age of emergence for the central incisor.
The mandibular permanent teeth tend to erupt before maxillary teeth. The mandibular central incisor usually erupts before the maxillary central incisor (and may erupt simultaneously with, or even before, the mandibular first molar. The mandibular lateral incisor may erupt along with the central incisor.
Before the permanent central incisor can come into position, the primary central incisor must be exfoliated. This is brought about by the phenomenon called resorption of the deciduous roots. The permanent tooth in its follicle attempts to force its way into the position held by its predecessor.
The pressure brought to bear against the primary root evidently causes resorption of the root, which continues until the primary crown has lost its anchorage, becomes loose, and is finally exfoliated. In the mean time, the permanent tooth has moved occlusally, so that when the primary tooth is lost, the permanent one is at the point of eruption and in proper position to succeed its predecessor.
The follicles of the developing incisors and canines are in a position lingual to the deciduous roots. The developing premolars which are to take the place of deciduous molars are within the bifurcation of primary molar roots. The permanent incisors, canines, and premolars are called succedaneous teeth. since they take the place of their primary predecessors.
Root resorption sometimes does not follow the routine procedure, with the result that the permanent tooth cannot emerge or else is kept out of its normal place. The failure of the deciduous root to resorb may bring about prolonged retention of the deciduous tooth
8 years Mandibular lateral incisors erupt very soon after the central incisors, often simultaneously. The maxillary central incisors erupt next in the chronological order, and the maxillary lateral incisors make their appearance about a year later.
10 years The first premolars follow the maxillary laterals in sequence when the child is about IO years old; the mandibular canines (cuspids) often appear at the same time.
12 years The second premolars follow during the next year, and then the maxillary canines follow. Usually. the second molars come in when the individual is about 12; they are posterior to the first molars and are commonly called “12-year molars." The maxillary canines occasionally erupt along with the second molars, but in most instances of normal eruption the canines precede them.
The third molars do not come in until the age of 17 years or later. Considerable jaw growth is required after the age of 12 to allow room for these teeth. Third molars are subject to many anomalies and variations. Insufficient jaw development for their accommodation complicates matters in the majority of cases.
Individuals who have properly developed third molars in good alignment are very much in the minority. Third-molar anomalies and variations with the complications brought about by malalignment and subnormal jaw development comprise a subject too vast to be covered here.
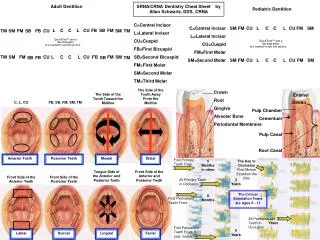
Development of the Teeth Apparently there are four or more centers of formation for each tooth. The formation of each center proceeds until there is a coalescence of all of them. Each of these centers (when referring to the crown portion) is called a lobe. Although no lines of demarcation are found in the dentin to show this development, there are signs to be found on the surfaces of the crowns and roots; these are called developmental grooves
After the crown of the tooth is formed, the root portion is begun. At the cervical border of the enamel, at the cervix of the crown, cementum starts to form as a root covering of the dentin. The cementum is hard tissue (similar in some ways to bone tissue) which covers the root of the tooth in a thin layer.
The junction of enamel and cementum is called the Cementoenamel junction. For descriptive purposes in dental anatomy, this is spoken of as the cervical line. forming a line of demarcation between the crown and root.
The development of the crown and root takes place within a bony crypt in the jaw bone. The development of the permanent teeth and resorption of the roots of deciduous teeth may be seen in periapical radiographs as well as panoramic radiographs
After the crown and part of the, root are formed, the tooth penetrates the mucous membrane and makes its entry into the mouth. Further formation of the root is supposed to be an active factor in pushing the crown toward its final position in the mouth.
Eruption of the tooth is said to be completed when most of the crown is in evidence and when it has made contact with its antagonist or antagonists in the opposing jaw. Actually, eruption may and usually does continue after this; i.e., more of the crown may become exposed and the tooth may move farther occlusally to accommodate itself to new conditions.
Formation of root dentin and cementum continues after the tooth is in use. The root formation is about half finished when the tooth emerges. Ultimately, the root is completed. Cementum covers the root.
The pulp tissue continues to function with its blood and nerve supply after the tooth is formed. The pulp cavity within the tooth has by this time become small in comparison with the tooth size. Its outline is similar to the outline of the crown and root, and the opening of the pulp cavity at the apex is constricted. This opening is called the apical foramen. The pulp keeps its tissue-forming function, in that it may form secondary dentin on occasion as a protection to itself.
Formation of the tooth is said to be completed when the apex of the root is formed; as a matter of fact, however. this process continues slowly throughout the life of the tooth. The pulp cavity becomes smaller and more constricted with age. Sometimes the pulp chamber within the crown is entirely obliterated. and in rare instances the entire pulp cavity has been found filled with secondary deposit.
This process is not so extensive in deciduous teeth, since the years of their usefulness are fewer; nevertheless, the same powers are inherent in the primary pulp. Primary teeth still show secondary dentin in their pulp chambers as a result of the irritation produced by caries or excessive wear.
The dental pulp is a connective-tissue organ containing a number of structures, among which are arteries, veins, a lymphatic system, and nerves. Its primary function is to form the dentin of the tooth. When the tooth is newly erupted, the dental pulp is large; it becomes progressively smaller as the tooth is completed.
The pulp is relatively large in primary teeth and also in young permanent teeth. For this reason, the teeth of children and young people are more sensitive than teeth of older people to thermal change and dental operative procedure