Download
1 / 1
10 likes | 272 Views
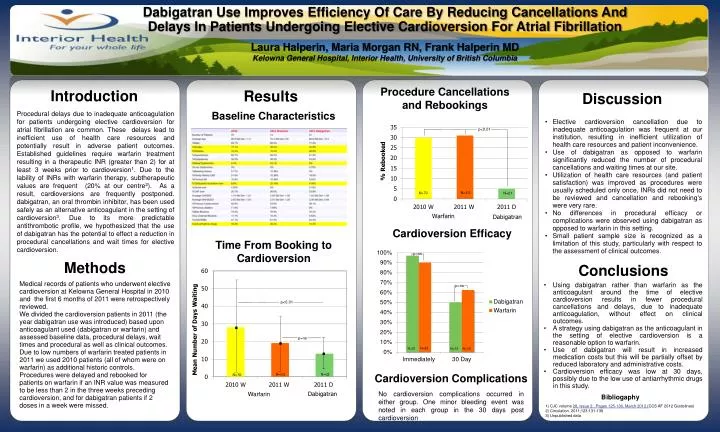
Dabigatran Use Improves Efficiency Of Care By Reducing Cancellations And Delays In Patients Undergoing Elective Cardioversion For Atrial Fibrillation Laura Halperin, Maria Morgan RN, Frank Halperin MD Kelowna General Hospital, Interior Health, University of British Columbia.

E N D
Dabigatran Use Improves Efficiency Of Care By Reducing Cancellations And Delays In Patients Undergoing Elective Cardioversion For Atrial Fibrillation Laura Halperin, Maria Morgan RN, Frank Halperin MD Kelowna General Hospital, Interior Health, University of British Columbia Procedure Cancellations and Rebookings Introduction Results Discussion Baseline Characteristics Procedural delays due to inadequate anticoagulation for patients undergoing elective cardioversion for atrial fibrillation are common. These delays lead to inefficient use of health care resources and potentially result in adverse patient outcomes. Established guidelines require warfarin treatment resulting in a therapeutic INR (greater than 2) for at least 3 weeks prior to cardioversion1. Due to the lability of INRs with warfarin therapy, subtherapeutic values are frequent (20% at our centre2). As a result, cardioversionsare frequently postponed. dabigatran, an oral thrombin inhibitor, has been used safely as an alternative anticoagulant in the setting of cardioversion3. Due to its more predictable antithrombotic profile, we hypothesized that the use of dabigatran has the potential to effect a reduction in procedural cancellations and wait timesfor elective cardioversion. • Elective cardioversion cancellation due to inadequate anticoagulation was frequent at our institution, resulting in inefficient utilization of health care resources and patient inconvenience. • Use of dabigatran as opposed to warfarin significantly reduced the number of procedural cancellations and waiting times at our site. • Utilization of health care resources (and patient satisfaction) was improved as procedures were usually scheduled only once, INRs did not need to be reviewed and cancellation and rebooking's were very rare. • No differences in procedural efficacy or complications were observed using dabigatran as opposed to warfarin in this setting. • Small patient sample size is recognized as a limitation of this study, particularly with respect to the assessment of clinical outcomes. p<0.01 N=70 N=21 Cardioversion Efficacy Time From Booking to Cardioversion Methods Conclusions Medical records of patients who underwent elective cardioversion at Kelowna General Hospital in 2010 and the first 6 months of 2011 were retrospectively reviewed. We divided the cardioversion patients in 2011 (the year dabigatran use was introduced) based upon anticoagulant used (dabigatran or warfarin) and assessed baseline data, procedural delays, wait times and procedural as well as clinical outcomes. Due to low numbers of warfarin treated patients in 2011 we used 2010 patients (all of whom were on warfarin) as additional historic controls. Procedures were delayed and rebooked for patients on warfarin if an INR value was measured to be less than 2 in the three weeks preceding cardioversion, and for dabigatran patients if 2 doses in a week were missed. • Using dabigatranrather than warfarin as the anticoagulant around the time of elective cardioversion results in fewer procedural cancellations and delays, due to inadequate anticoagulation, without effect on clinical outcomes. • A strategy using dabigatranas the anticoagulant in the setting of elective cardioversion is a reasonable option to warfarin. • Use of dabigatran will result in increased medication costs but this will be partially offset by reduced laboratory and administrative costs. • Cardioversion efficacy was low at 30 days, possibly due to the low use of antiarrhythmic drugs in this study. p<0.01 p=ns N=83 N=12 N=13 Cardioversion Complications N=21 N=70 No cardioversion complications occurred in either group. One minor bleeding event was noted in each group in the 30 days post cardioversion Warfarin Bibliogaphy 1) CJC volume 28, Issue 2 , Pages 125-136, March 2012 (CCS AF 2012 Guidelines) 2) Circulation. 2011;123:131-136 3) Unpublished data