Download
1 / 15
150 likes | 314 Views
Cardioversion turns 50. Seth Bilazarian MD Private practice theheart.org. "A new electronic method". 50 years ago today, Lown et al described cardioversion as a "new electronic method". http://www.nejm.org/doi/full/10.1056/NEJM196308152690701. A lot hasn't changed.

E N D
Cardioversion turns 50 Seth Bilazarian MD Private practice theheart.org
"A new electronic method" • 50 years ago today, Lown et al described cardioversion as a "new electronic method" http://www.nejm.org/doi/full/10.1056/NEJM196308152690701
A lot hasn't changed • Atrial fibrillation: • Is the most prevalentof the chronic rhythm disorders of the heart • Increased tendency to systemic and pulmonary emboli • Impairs cardiac performance • New method was designated "cardioversion" http://www.nejm.org/doi/full/10.1056/NEJM196308152690701
Some things have changed • The method of terminating AF has not changed since Frey introduced quinidine in 1918 • Quinidine commonly produces untoward reactions that range from gastrointestinal upset to sudden death. The American literature alone has documented 26 deaths up to 1956 http://www.nejm.org/doi/full/10.1056/NEJM196308152690701
Single limitation is the need for anesthesia. Patient is usually unconscious for 2-5 minutes, procedure completed in 15-30 minutes. • Cardioversion is safe: • When DC pulse is synchronized to discharge outside the ventricular vulnerable period, the possibility of fibrillation is entirely prevented • EKG before and after reversion showed no change in the ventricular complex. • In a few patients persistent sinus bradycardia, episodic nodal rhythm and atrioventricular dissociation occurred. These either were the result of overdigitalization or perhaps represented depression or pre-existing injury of the sinus node. • Definite but small risk of embolism with any reversion of AF to normal rhythm. Therapy is carried out for a period of 3 weeks before and 1 week after cardioversion. What else hasn't changed? http://www.nejm.org/doi/full/10.1056/NEJM196308152690701
"This procedure has been designated as cardioversion, and the instrument is referred to as a cardioverter." One name caught on, one didn't http://www.nejm.org/doi/full/10.1056/NEJM196308152690701
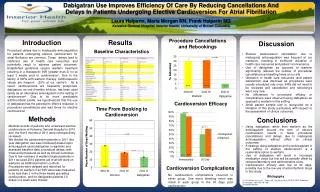
Medicare claims data analyses Source: 2008 to 2012 Medicare Physician Fee Schedule, national average (unadjusted) rates. 2008 to 2012 Medicare Physician Claims Database (100% sample). Created by Dr Seth Bilazarian
Medicare claims data analyses Source: 2008 to 2012 Medicare Physician Fee Schedule, national average (unadjusted) rates. 2008 to 2012 Medicare Physician Claims Database (100% sample). Created by Dr Seth Bilazarian
Medicare claims data analyses Source: 2008 to 2012 Medicare Physician Fee Schedule, national average (unadjusted) rates. 2008 to 2012 Medicare Physician Claims Database (100% sample). Created by Dr Seth Bilazarian
Decline in our use of cardioversion Source: Dr Seth Bilazarian
Growing because: • AF increasing with aging population and increase in obesity • Ease of TEE and cardioversion • "Part" of the AF ablation treatment algorithm Not growing as fast: • Comfort with rate control alone in asymptomatic patients • Use of ibutilide(Corvert) as an alternative Contributing to the numbers
Management of AF with the rhythm-control strategy offers: • No survival advantage over the rate-control strategy • Potential advantages, such as a lower risk of adverse drug effects • Anticoagulation should be continued in this group of high-risk patients AFFIRM Trial 12/15/2002 • http://www.nejm.org/doi/full/10.1056/NEJMoa021328
Rate control: • Safe, negative chronotropic drugs, anticoagulation • Symptoms? • AV nodal ablation and pacing Rhythm control: • Drugs • Cardioversion • Drugs then cardioversion • AF ablation Options for the AF Patient
Procedure lasts 90 minutes to four hours • 30% to 40% chance it will need to be repeated • Works about 80% of the time for three to five years but higher likelihood of recurrence beyond five years • Procedure-related risks • Will not change the need for anticoagulation • This is not curative, it's palliative AF ablation: Pre–EP-consult consent
Effective nontoxic drug therapy for maintenance of sinus rhythm. We have: • Effective and toxic • Ineffective and safe • Ineffective and toxic • Better definition of who will best benefit by AF ablation (predicted to be $2.4 billion in 2021) and improvement in acute success and durability Still unmet need


![Sankoff turns 50!! Using Spannoids [k-restricted Steiner Trees] for Sequence Analysis](https://cdn1.slideserve.com/2222089/slide1-dt.jpg)