Download
1 / 17
170 likes | 297 Views
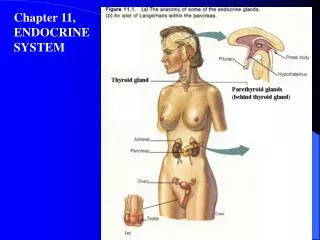
Caring for client’s with Endocrine DO. Bakersfield College VN 86 PP #2. Pituitary Gland. Pituitary disorders less common than other disorders although can cause diverse and serious problems.

E N D
Caring for client’s with Endocrine DO. Bakersfield College VN 86 PP #2
Pituitary Gland • Pituitary disorders less common than other disorders although can cause diverse and serious problems. • Hyperpituitarism- excess production and secretion of one or more hormones. Commonly causes oversecretion of growth hormone. • Hypopituitarism- lack of production of one or more of the gland’s hormones • Pituitary tumors usually cause both of these conditions.
Pituitary Gland Anterior • Growth hormone is produced by the anterior lobe of the pituitary gland. It stimulates growth of the long bones • Excess secretion of GH prior to puberty and the closure of the epiphyseal plates causes gigantism. These patients can be over 7 foot tall. • Dwarfism occurs when there is an inadequate production of GH during childhood. • During adulthood bones and connective tissue grow at a slow rate and cause things like enlarged forehead and protruding jaw. Hypersecretion during adulthood. • Untreated: HTN, DM cardiac enlargement and failure.
Pituitary • DX: MRI and CT show enlargement along with tumor. • Labs show elevated growth hormone levels. • Pituitary tumor treated with transphenoidal hypophysectomy removal of the pituitary gland • Irradiation of the pituitary tumor • Drug therapy with Sandostatin (octreotide) decreases growth hormone production does not reduce tumor size. • Lifelong hormone replacement therapy needed.
Posterior Pituitary Gland • Disorders of the posterior pituitary are caused by too much or too little antidiuretic hormone (ADH). • ADH regulates total body water by acting on the kidney to retain or release water. • Receptors in the Hypothalamus control the release of ADH in response to serum osmolarity. • Remember: • When serum osmolarity increases ADH secretion increases and renal water is reabsorbed, which decreases urine output. • When serum osmolarity decreases (hyposmolarity)it suppresses the release of ADH so urine output increases. • Thus:
Diabetes Insipidus • DI results from ADH insufficiency. Two types: • 1. Neurogenic DI- results from damage to the pituitary gland after head injury or cranial surgery. • 2. Nephrogenic DI- kidneys fail to respond to ADH secretion due to renal failure. • Deficient supply of ADH causes a urinary output of 5 to 15 liters per day. Client develops polydipsia. If the patient can not replace the water loss dehydration develops. • Risk for hypernatremia. • See manifestations:
DI Diabetes insipidus diagnosis is based on presence of CM, risk factors, water deprivation test see textbook. • Treatment: • Replace the water loss IV 0.45 NS • ADH replacement therapy DDAVP or vasopressin • Sodium restriction and thiazide diuretics for nephrogenic DI
SIADH • Syndrome of inappropriate ADH secretion • Results from excess production of ADH. • Caused by lung tumor, head injury, pituitary surgery use of barbiturates, anesthetics or diuretics. • Excess production of ADH leads to water retention hyponatremia and serum hyposmolarity. • CM- decreases urine output and concentrated urine. • Neurologic symptoms- cells in the brain swell as water moves in. • No edema in body, water is going to the extracellular spaces
SIADH • Treatment- correcting the underlying cause, limit fluid intake so fluid will go back into the cells. • Diuretics such as lasix, with fluid restriction. • Meds: • Declomycin to promote urine producion • Hypertonic saline. • CM- see text • Why fluid restriction?-prevents further dilution of the plasma and sodium levels. • Diuretics will help to decrease fluid volume excess • Seizure precautions: low serum sodium levels can lead to seizures. • Teaching- fluid restriction at home and medications. Video
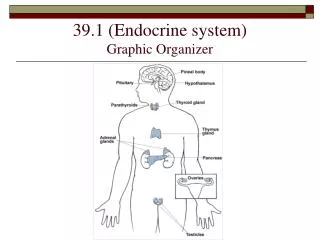
Adrenal Gland Disorders • Disorders involve either the adrenal cortex- secretes cortisol and aldosterone. • Or the Adrenal medulla- Releases epinephrine and norepinephrine. • Can cause physical, psychologic and metabolic alterations that can be life threatening. Most common d/o are • 1. Cushing’s syndrome, Addison’s disease and pheochromocytoma.
Cushing’s Syndrome • Chronic disorder in which the adrenal cortex produces excessive amounts of the hormone cortisol. • More common in women 30-50 yrs. May be caused by: • Adrenal tumors • Tumor of the pituitary gland which increases ACTH release which stimulates the adrenal cortex to produce cortisol. • Chronic glucocorticoid therapy- Where do we see this? • Increased release of ACTH from certain tumors. Lung, pancreatic.
Cushing’s Syndrome • Too much cortisol/glucocorticoids result in changes in CHO metabolism, protein and fat metabolism. • Fat deposits • Buffalo hump • Moon face • Muscle weakness and wasting • Loss of collagen and connective tissue, thus poor wound healing • Thin skin with striae • DM may occur. • Osteoporosis compression fractures • Hypertension, infection, peptic ulcers, depression, hirsutism.
Cushing’s Syndrome • Treatment: • Surgery radiotherapy or medication • Pituitary adenoma- surgery • Radiation if inoperable tumor • Drug therapy when surgery is contraindicated. • DX test: increased plasma cortisol level / elevated 24 hour urine test for 17 ketosteroids and 17 hydrocorticosteroids. • Plasma ACTH levels are elevated when caused by pituitary gland tumor • Serum sodium and glucose levels are elevate in Cushing’s Syndrome.
Cushing’s Syndrome • If surgery indicated when adrenal cortex tumor. • Usually only one adrenal gland is involved. • If both taken the client will have to take lifelong corticosteroid and mineralcorticoid replacement therapy. • Addisonian crisis is risk after both glands removed. • Radiation therapy when client has inoperable pituitary tumor causing Cushing’s syndrome. • Radioactive isotopes implanted into the pituitary gland. Lifelong replacement of hormones • See Nursing Care.
Addison’s Disease • Most common form of adrenal cortex insufficiency. • Women under age 60. • Primary- Adrenal cortex hypofunction. Autoimmune response. Which destroys the client’s own adrenal cortex. • Secondary- Lack of pituitary ACTH.adrenalcorticotropic hormone • DX: decreased serum levels of cortisol, atrophy of adrenal gland on CT. • Manifestations are slow CM when 90% gland destroyed. • CM are from elevated ACTH levels and decreased aldosterone and cortisol. Primary complication is Addisonian crisis. • CM- See text • Tx: early diagnosis, cortisol replacement, this can induce Cushing’s syndrome. See textbook.
Addisonian Crisis • Serious life threatening response to acute adrenal insufficiency. • Major stressors precipitate the condition. • May occur in clients who abruptly withdraw corticosteroid medications • CM- hypotension, rapid weak pulse, extreme weakness, confusion, altered K levels, cardiac dysrhythmias. • TX: IV fluids, glucose, sodium glucocorticoids.
Adrenal Medulla Disorders • Pheochromocytoma- benign tumor of the adrenal medulla. • Middle aged adults • Produces excessive amounts of catecholamines such as epinephrine or norepinephrine. • This stimulates the sympathetic nervous system which in turn • Leads to dramatic rise in the systolic blood pressure!! • 200/150. • Can lead to stroke and MI • DX: increased catecholamine levels in the blood. • CT or MRI • TX: Surgical removal; laparoscopic adrenalectomy • NR; Blood pressure,adrenal hormone replacement therapy, hypertension may be a problem chronic.