Download
1 / 45
550 likes | 1.57k Views
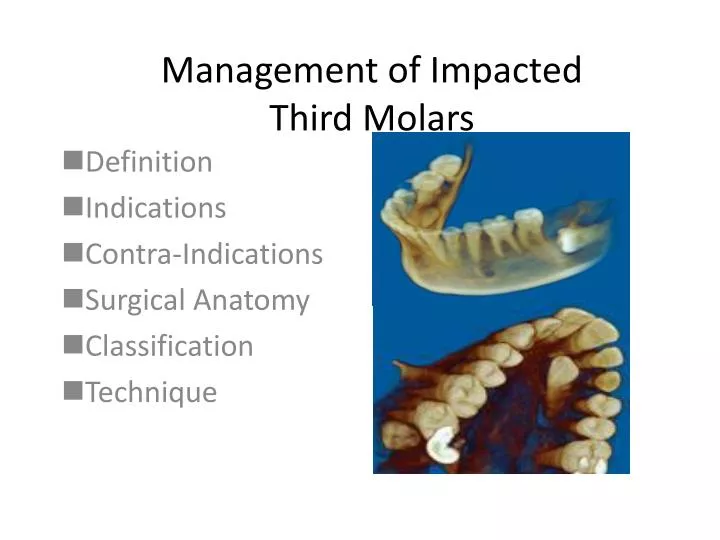
Management of Impacted Third Molars. Definition Indications Contra-Indications Surgical Anatomy Classification Technique. Terminology. Impacted – An impacted tooth is one that fails to erupt into the dental arch within the expected time.

E N D
Management of Impacted Third Molars Definition Indications Contra-Indications Surgical Anatomy Classification Technique
Terminology • Impacted – • An impacted tooth is one that fails to erupt into the dental arch within the expected time. • Unerupted includes both impacted teeth and those that are in the process of erupting • Embedded- • This is occasionally used interchangeably with the term impacted
Definition of Impaction • A tooth which is completely or partially unerupted and is positioned against another tooth, bone, or soft tissue so that its further eruption is unlikely, described according to its actual anatomic position. -Archer
Causes • Inadequate space • Inadequate dental arch space • Inadequate space for eruption • Obstruction to normal path of eruption • Lack of skeletal development • Mandibular retrognathia • Congenital disorders
Failure of third molars to upright • Normal development • Failure of coordinated eruption • Stunted growth of the tooth germ • Severe nutritional deficiency • Irradiation • Physical trauma
Frequency • Last teeth erupting in available space • Mandibular & Maxillary Third molars • Maxillary Canines • Mandibular premolars
Why and When? • The indications for removal of asymptomatic impacted third molar has been challenged. • Do the risks and costs accumulated from extraction outweigh the life long benefits of their removal ?
Indications • Prevention of • Pericoronitis • Periodontal disease • Root resorption • Cyst formation • Caries • Prosthetic consideration • Fracture of Mandible • Pain of unexplained reason • Other considerations • Orthodontic
Prophylactic removal • Is there a need? • Clinical questions that help us address this issue
Clinical questions? • Can we predict the course of eruption of an Unerupted third molar? • Unpredictable • Guiding factors • adequate space • Radiographic evaluation • Impacted molars after the age of 25 may still change in position
Clinical questions? • Does the presence of third molar affect the periodontal health of the adjacent second molar? • Third molars adversely affects the periodontium of adjacent second molars • Greater probing depths
Clinical questions? • Does the removal of third molar affect the periodontal health of the adjacent second molar? • impacted third molars can negatively impact the periodontium of adjacent second molars. • Factors: • preoperative presence of an intrabony defect, • age of the patient, • level of plaque
Does presence of third molar influence the progression and severity of periodontitis? • Greater probing depths before and after extraction • Visible third molars • >5 mm probing depths progression is more • Effectiveness of periodontal therapy is affected adversely • Chances of future progression are bright
Optimal Periodontal Healing • Preserve periodontal health of 2nd molar • Bone height on distal aspect of second molar • Periodontal Attachment • Two major factors • Extent of the preoperative infrabony defect • Age of the patient • Asymptomatic completely bony impacted 3rd molar should not be extracted in a patient of >30years of age.
Does Age play a role? • Presence of third molars and age • Late erupting teeth have pathology • Periodontal Pathology and age • Increased prevelence • Caries and age • Increase prevalence with increasing age • Postoperative risks and age • >morbidity in patients over 25years
Evidence in support of prophylactic removal • Extensive evidence that supports prophylactic removal • Asymptomatic and radiographically pathology free retained 3rd molars do pocess a potential of cystic /neoplastic transformation • Periodontal disease and its link with systemic disease • Odontogenic infections
Ideal time for extraction of Impacted teeth • Average age: 20years • Ideal time for extraction • When the roots are 1/3 formed and before they reach 2/3 formation • Early removal • Low morbidity • Tolerate procedure better • Quick recovery
Cyst Formation • Low Incidence • High morbidity • Dental Follicle may undergo cystic changes • >3mm = cyst • Types • Dentigerous cyst • Keratocyst
Tumor formation • Odontogenic tumors • Ameloblastoma
Should asymptomatic impacted molars under an existing or planned prosthesis be removed? • Removal indicated before Prosthetic appliance is constructed • Decision will be based on • Age • Position • Degree of difficulty • Type of prosthesis
Pain of Unexplained origin & jaw fractures • Unexplained pain, in the retro molar region (TMD is excluded) • Prevention of jaw fractures
Orthodontic considerations • Distalization of first and second molars • Crowding of mandibular anterior teeth • Multifactorial • 3rd molars may play a significant role but cannot be sole cause
What is the microflora around the 2nd and 3rd molars? • Microflora detected in gingival crevice around 3rd Molars • Alpha hemolytic streptococci • Prevotella • Veillonella • Bacteroides • Capnocytophaga
Pericoronitis • Definition • Pericoronitis is an infection of the soft tissue around the crown of a partially impacted tooth and is caused by the normal oral flora. • Causes • Imbalance between host defenses • Minor trauma • Food entrapment
Pericoronitis More common in Mandibular 3rd molars than Maxillary 3rd Molars
Pericoronitis • Organism responsible- streptococci (anaerobic) • Types • Acute • Chronic • Or • Mild (localized tissue swelling and soreness) • Moderate ( large amount of soft tissue swelling, purulent discharge • Severe ( Facial space infection, severe pain, trismus, low grade fever)
Pericoronitis -Signs and Symptoms • Pain • Swelling • Inflammation • Purulent discharge • Trismus • Temperature
ACUTE Pericoronitis • Timing of Extraction for third molar • Defer until all symptoms are completely resolved • Minimum 7 days of antibiotics • Why should we defer? • Virulent bugs • Extensive Surgery • High morbidity if infection spreads
Findings: Acute • Severe Pain • Inflammation, swelling • around the impacted • or erupted tooth • Trismus • Traumatic ulceration • Facial swelling • Dysphasia • Lymphadenopathy Improvement Extraction • Treatment: • Irrigation • Saline/h2O2 • Debridement • Analgesics • Mouth rinses • Antibiotics • Change • antibiotic • C&S • chlorhexidine • Hospitalize • (if facial • Infection) No Improvement Acute Types Pericoronitis Simple extraction Improvement Extraction Chronic • Findings: Chronic • Low grade • gingival • Inflammation • Asymptomatic • Treatment: • Irrigation • Saline/h2O2 • Debridement • Analgesics • Mouth rinses • Antibiotics? Improvement Difficult extraction
Contra-indications • Extreme of age • Too young <10years • Too Old>40 years • Just right 16-28 years • Medically compromised status • Damage to adjacent structures • Periodontal • Loss of tuberosity • Adjoining teeth • IAN,Lingual Nerve • Sinus
Imaging Digital radiograph (X-ray) of the mandible of Magdalenian Girl showing impaction of the right lower third molar (wisdom tooth). New high-quality radiographic imaging of the entire Magdalenian Girl skeleton, which is 13,000 to 15,000 years old, has made reanalysis of this skeleton possible. (Photo courtesy of The Field Museum)
Imaging • Panoramic Radiograph-Gold standard • Identify the presence of third molars • Locate unusual position • Facilitate establishing angulation • Show vertical relationship to second molar • Identify caries and dentoalveolar bone loss • Detect location of IA canal • Detect Bone pathology • Establish height of the bone • Identify structural stability of the second molar
Imaging • Cone Beam CT & 3D Imaging
Risk assessment factors • Age • Obesity • Large tongue • Dilacerated roots • Strong gag reflex • Complaining patient • Location of the IAN • Surgical access space • Bone mass density • Dense Bone • Interincisal opening • Third molar position
References • Contemporary Oral and Maxillofacial Surgery; 5th edition, Hupp,Ellis,Tucker • White paper on third molar data(AAOMS March 2007)