Download
1 / 27
300 likes | 1.5k Views
Management of substernal goiter. UCH KH Tse. Clinical scenario. 70/F Asymptomatic. Refer for your expert opinion. Questions. What is the diagnosis ? How do you manage ?. Introduction. SSG First described by Haller in 1749. Account for 10-15% of all the mediastinal mass.

E N D
Management of substernal goiter UCH KH Tse
Clinical scenario • 70/F • Asymptomatic. • Refer for your expert opinion.
Questions What is the diagnosis ? How do you manage ?
Introduction • SSG • First described by Haller in 1749. • Account for 10-15% of all the mediastinal mass. • SSG / All thyroidectomy = 2.6-20% Madjar Chest 1995
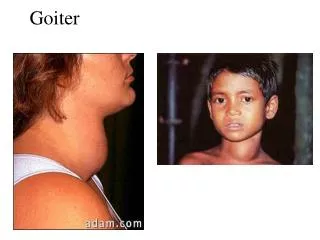
Definition • Confused. • Decend inferior to the thoracic inlet. Katlic et al Am J Surg 1998 2. >50% thyroid mass inside the thorax. Wax et al J Otolaryngol 1992 Arici et al Int Surg 2001 • Goitres extend to 4th thoracic vertebra. Lindskog and Goldenberg JAMA 1957
Anatomy SSG classified into two groups. • Truly intrathoracic or aberrant goiter (1%). • Congenital • Blood supply derived from the intrathoracic vessel entirely. • No connection to the cervical thyroid gland. Lahey & Swinton et al 1934
Anatomy 2. Arises in the cervical thyroid gland • Acquired. • Decends along a fascial plane through the thoracic inlet to the mediastinum. Lahey & Swinton et al 1934
Anatomy Anatomical constrain. Downward traction
Symptomatology • Neck mass, SOB, dysphagia. • 5-50% can be asymptomatic on presentation. Katlic MR Am J Surg 1985 • Prolong course of symptoms. • From 2 weeks to 20 years with symptoms before referral. Mean = 31 months.
Rationale for operation 1. SSG is progressive, can result in sudden airway obstruction. Singh B Am J Otolaryngol 1994. 2. Inaccessible to, inaccurate, and dangerous biopsy. Rietz KA Acta Chir Scand 1960 3. Long history MNG does not preclude malignancy, hyperfunction or complication. Malignancy in 7-17% Sanders Arch Surg 1992 Torre G Am Surg 1995
Rationale for operation • No effective alternative treatment. I131? T4? Allo MD Surgery 1983 • Less operative complication in the asymptomatic patients. Para-Menbrives et al Internat Surg 2003 The consensus is that substernal goiter is best managed surgically. Katlic MR Am J Surg 1985
Investigation CT neck and thorax is the most valuable. Netterville et tal Laryngoscope 1998 Sanders LE Arch Surg 1992 • Outline the extent of thyromegaly. • Differentiate the origin of the goiter. • Measure the degree of narrowing of the trachea.
The operation • Head up, neck well extended. • Wider and lower incision. • Division of the strap muscles. • Control cervical blood supply first. • Excise the opposite lobe first, to provide more room in the neck. Wheeler M.H. et al BJS 1999 • Sternotomy rate 2-11.7 % Michel LA Br J Surg 1988
The operation Other indications for sternotomy / thoracotomy • Intra thoracic goitre / ectopic goitre. • Vasoagressive signs. • Retroesophageal goiters. • Suspected malignancy, mediastinal lymphadenectomy. • After a prior cervical thyroidectomy, with intra-thoracic recurrent.
Our study Retrospective study • From Jan 2000 to Dec 2003 • 287 cases of thyroidectomy. • 24 (8.4%) were SSG • M:F = 5:19 • Mean age 60.1+/-15.5 (26 - 90)
Symptoms in patients with substernal goitre Symptoms & signsNumber(%) SOB (including 3 cases of acute airway obstruction) 8(33.3) Neck discomfort 1(4.2) Dysphagia 1(4.2) Hoarseness 1(4.2) Asymptomatic 13(54.2) Duration of symptoms 2-120 months, mean 43.3 +/- 47.5
Histopathologic diagnoses of substernal goitre Diagnoses Number(%) Hyperplastic nodules/nodular hyperplasia 18(75) Diffuse hyperplasia 2(8.3) Hurthle cell adenoma 1(4.2) Papillary carcinoma 1(4.2) Follicular carcinoma 1(4.2) Medullary carcinoma 1(4.2)
Morbidity of thyroidectomy for substernal goitre(N=24) Number(%) Recurrent laryngeal nerve injury(nerve at risk) 1(2.7) Transient hypoparathyroidism(patients at risk N=15) 2(13.3) Permanent hypoparathyroidism 0 Haematoma 1(4.2) Wound infection 1(4.2) Pneumonia 1(4.2) Motality 0
Comparison of complications between asymptomatic and symptomatic patients Complications Asymptomatic (13) Symptomatic (11) Recurrent laryngeal nerve injury 0 1 Transient hypoparathyroidism 1 1 Haematoma 0 1 Pneumonia 0 1 Wound infection 0 1 Fisher exact test, p=0.033 Para-Menbrives et al Internat Surg 2003
Conclusion A substernal goiter is always indicated for resection and should be performed early, except the patient is unfit for operation.
Comparison of asymptomatic vs. symptomatic patients Asymptomatic(N=13) Symptomatic(N=11)p Age(yr) 55.3 65.7 0.10 Gender(F/M) 10/3 9/2 0.79 Toxic goitre/non-toxic goitre 9/4 9/2 0.60 Duration of presentation(month) 38.2 38.0 0.98 Hemithyroidectomy/bilateral resection 5/8 6/5 0.53 Previous thyroid surgery(Yes/No) 13/0 9/2 0.11 Elective/emergency operation 13/0 9/2 0.11 Benign/malignant histopathology 12/1 9/2 0.54 Specimen weight(gm) 213.2 174.5 0.47 Parathyroid autograft(Yes/No) 3/10 3/8 0.81 Operative blood loss(ml) 194.9 223.8 0.86 Duration of surgery(min) 178.8 196.8 0.60 Postoperative hospital stay(days) 3.2 6.3 0.08
Our study Reasons for more complication in the symptomatic group. • Patient is older. • More emergency operation. • May be a larger proportion of the goitre is intrathoracic.