Download

1 / 66
670 likes | 1.25k Views
Cutaneous Malignant Neoplasm in brief. Prof ME Akbari. Cutaneous Malignant Neoplasm in brief. BCC SCC Malignant Melanoma Dermatofibrosarcoma Extra mammary Paget dis Angio sarcoma Kaposi Sarcoma

E N D
Cutaneous Malignant Neoplasm in brief Prof ME Akbari
Cutaneous Malignant Neoplasm in brief BCC SCC Malignant Melanoma Dermatofibrosarcoma Extra mammary Paget dis Angio sarcoma Kaposi Sarcoma Merkel Cell Carcinoma(rare,viral,fatal)
Cutaneous Malignant Neoplasm in brief Etiology Sun Light SCC/BCC more and less in Melanoma Genomics KIT20%/BRAF50%/NRAS 15%/ MAPK(mitogene activated protein kinase) More in Melanoma less in others
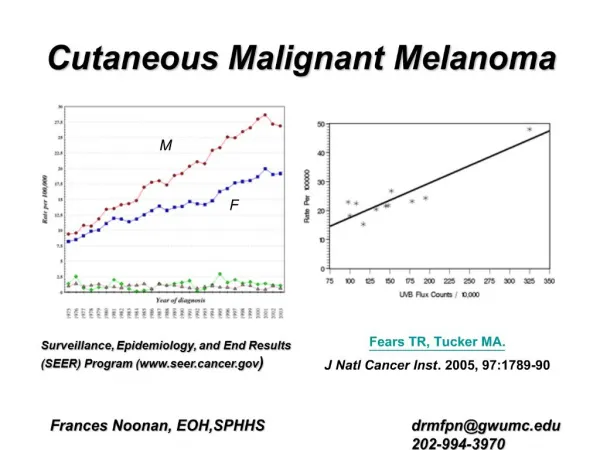
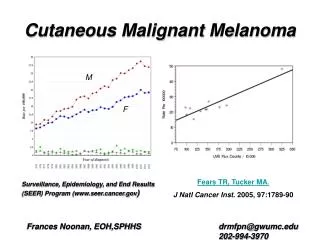
Malignant Melanomain brief Melanoma is around 2% of all skin Malignancies in west and 4% in Iran.
Malignant Melanomain brief Melanoma cause the majority of skin cancer related death
Hallmark Steps in development of Melanoma 1-self sufficient growth signaling 2-Evasion of tumor suppressor signals 3-down regulation of Apoptosis 4-Unlimitted replication 5-Sustained angiogenesis 6-progression to invasion and metastasis 7-…………………
Clinical Suspicious of diagnosis-Melanoma ABCDEs Asymmetry Border Irregular Color change Diameter greater than 6 mm Evolution(change over time)
Best Evaluation singe of Melanoma History and physical examination (undress by family) Change over time Ulceration Bleeding
Biopsy in Melanoma principle Complete skin thickness and thickened site 1- Excisional biopsy for small lesions 2-Punched bx or incisional bx from thickened site 3-Minimum diameter of specimen 4mm 4-shave bx suitable for nonmelanotic melanoma
Melanoma Pathology management Insitu WLE with 0/5-1 cm free margin Invasive Complex Management
Melanoma Characteristic Acral Lentiginous Melanoma
730 Acrallentiginious
1-superfitial spreading melanoma 2- nodular 2 1
Staging Melanoma 1-Previous Slides 2-Stage I & II No more evaluation such as LFT or LDH and Imaging 3-IIIa (SLN is positive only) No need for imaging 4-IIIb/c Need Imaging
Surgery • 734
SLNB in Melanoma IN 20/8% there is differences between SLNB and observing lymph nodes.
SLNB in Melanoma 1- No need in all thin (<1mm) cases 2-in thin cases but high mitotic index (>=1 mitosis/ mm2) it is recommended when it is high mitotic the stage will change from T1a to T1b 3-young ages (<40) and male sexes are risk factors and more indicated for SLNB 4- clark level alone is not indicated for SLNB but with other factors such as age and sex with level iv and v are indicated. 5-SLNB in thick melanoma (Breslow >=4mm) will affect OS DFS and recommended 6-SLNB will help to detect the unknown real drainage site
Melanoma in Medial site of Rt Hand SLN is positive in both site Plan?
Lymph Node Treatmentin Melanoma IN Case of LN+ Lymphadenectomy is mandatory it will improve OS and DFS Radical lymphadenectomy is suitable for Malignant Melanoma for example: Breast max LAXLND but for Melanoma Drained in Axilla minimum Level I, II, III
Lymph Node Treatmentin Melanoma Inguinal SLN+ = Superficial Lymphadenectomy Pelvic Dissection not recommended ?? But Pelvic Metastasis Lymphadenectomy pelvic is recommended
Lymph Node Treatmentin Melanoma Cervical Lyphadenectomy Functional Lymphadenectomy Preserve Nerve and Vein Parotid Only guided by SLN
Lymph Node Treatmentin Melanoma Axilla and Epitrocheal Inguinal and Popliteal Epitrocheal & Popliteal not recommend in all cases If Inguinal and Axilla are Negative ??
Adjuvant Therapyin Melanoma 25 Trials iii No benefit from Chemotherapy and Immune stimulant New NCCN guideline : Interferon and Radiation in stage II and III in selected cases Interferon @-2b 12 months First month high dose Then 3 times weekly
RT in Melanoma In some selected cases with Nodal involvement
MelanocyteOrigin and Location • Originate from Neural Crest • Migration to Epidermis • Secretion of Melanin • Distribute among Keraniocyte • (1/10 and 500 – 2000 cells / mm2)
Non Melanoma Skin Cancer Most prevalent up to 95% In Iran and more in West Sun light important risk factor 10 to 65 fold in immunosuppressive cases such as Transplant Don,t forget the high risk cases (addiction)
Non Melanoma Skin Cancer BCC SCC Dermatofibrosarcoma Extra mammary Paget dis Angio sarcoma Kaposi Sarcoma Merkel Cell Carcinoma(rare,viral,fatal)
BCC Surgery _Moh,s Microsurgery _Excisional Surgery _Cautery and destruction
SCC Surgery WLE/SLNB…/lymphadenectomy Margin +/ Not suitable surgery Neo Adjuvant Chemoradiation
SCC Chronic Ulcer
SCC LIP SCC
LIP SCC Radical Neck after positive Sentinel Node
Biopsied= SCC