Download
1 / 18
180 likes | 506 Views
Quality Improvement Project to Develop a Telephone Protocol to Triage Vaginitis Complaints in Adult Non-pregnant Patients. Ann Evensen, MD UW Health Monona November 6, 2008. Question 1.

E N D
Quality Improvement Project to Develop a Telephone Protocol to Triage Vaginitis Complaints in Adult Non-pregnant Patients Ann Evensen, MD UW Health Monona November 6, 2008
Question 1 22 y/o unmarried female in long term monogamous relationship calls with vulvar itching, swelling and dysuria for the past three days. Has tried nothing at home. Wants diflucan called in.
Treatment options A) Treat with Diflucan over the phone B) Treat with metronidazole over the phone C) Treat with Monistat over the phone D) Treat with sulfa over the phone E) Schedule office visit for evaluation F) Other?
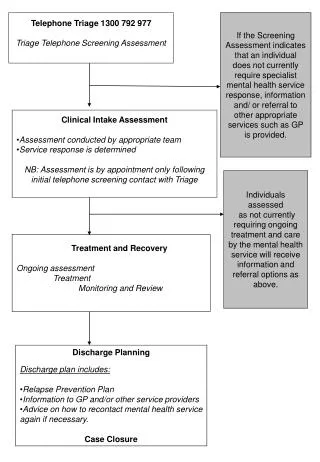
Project Objective • Develop a protocol for telephone triage of vaginitis complaints from non-pregnant, adult females
Triage Protocol Design • Literature review • Assessment of our clinical practice • Stakeholder input
Literature review Previously created protocols Sensitivity and specificity of signs and symptoms Correlation between telephone and in-person interviews
Assessment of clinical practice • Spreadsheet of 5 telephone encounters from each physician and NP (total of 30 calls) • Summarized phone advice given and any related visits next two months
Pilot protocol • Evidence based material • Expert opinion • Took previously summarized calls and put them through pilot protocol
Meetings with stakeholders • Met twice with doctors, nurses, MAs and front desk staff • Presented info on vaginitis diagnosis • Listened to their concerns and preferences
EMR installation • Created a Smart Phrase of protocol in our electronic medical record (“EPIC”) • Recruited computer-savvy nurse to assist in loading Smart Phrase in all staff computers
Protocol Revisions • Regularly checked in with staff regarding their opinions and patient feedback after trying protocol • Many found protocol too long
User feedback • Keep/revise – 2/3 • Toss – 1/3
Lessons learned • Practices vary considerably • “Expert opinion” vs EBM • Implementation requires buy-in • Success requires feedback and revision
Conclusion • Vaginitis diagnosis difficult : low predictive value of signs and symptoms. • Protocol can be developed for an urban family medicine clinic • treat a few patients over the phone • avoid delay in scheduling office visits • decrease uncompensated physician time
Future Does this protocol simply help clinic triage issues or does it lead to more accurate diagnosis and appropriate treatment of women with vaginitis symptoms?