Download
1 / 23
230 likes | 269 Views
Learn about classification, pharmacokinetics, mechanisms of action, and toxicity of key skeletal muscle relaxants. Explore the use, interactions, and reversal of neuromuscular blocking drugs.

E N D
Haitham M. KADHIM Ph.D Pharmacology & Therapeutics COLLEGE OF MEDICINE AL-NAHRAINUNIVERSITY Skeletal Muscle Relaxants
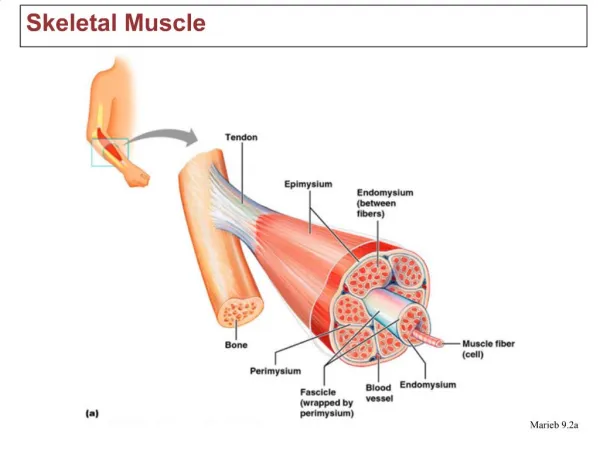
A) Neuromuscular Blocking Drugs Classification and Prototypes Skeletal muscle contraction is evoked by a nicotinic cholinergic transmission process. Blockade of transmission at the end plate is clinically useful in • producing muscle relaxation, a requirement for surgical relaxation, tracheal intubation and control of ventilation. Skeletal Muscle Relaxants
A) Neuromuscular Blocking Drugs Classification and Prototypes The neuromuscular blockers are quaternary amines structurally related to acetylcholine (ACh). Most are antagonists (nondepolarizing type), and the prototype is tubocurarine. One neuromuscular blocker used clinically, succinylcholine, is an agonist at the nicotinic end plate receptor (depolarizing type). Skeletal Muscle Relaxants
A) Neuromuscular Blocking Drugs 1) Nondepolarizing Neuromuscular Blocking Drugs Pharmacokinetics i)All agents are given parenterally. ii) They are highly polar drugs and do not cross the blood-brain barrier. iii) Drugs that are metabolized (eg, mivacurium, by plasma cholinesterase) or eliminated in the bile (eg, vecuronium) have shorter durations of action (10–20 min) than those eliminated by the kidney (eg, pancuronium, pipecuronium, and tubocurarine) which usually have durations of action of less than 35 min Skeletal Muscle Relaxants
. 1) Nondepolarizing Neuromuscular Blocking Drugs Pharmacokinetics iv)In addition to hepatic metabolism, atracurium clearance involves rapid spontaneous breakdown to form laudanosine and other products. At high blood levels, laudanosine may cause seizures. v) Cisatracurium, a stereoisomer of atracurium, is also inactivated spontaneously but forms less laudanosine and currently is one of the most commonly used muscle relaxants in clinical practice. Skeletal Muscle Relaxants
1-Nondepolarizing Neuromuscular Blocking Drugs _Mechanism of Action Nondepolarizing drugs prevent the action of ACh at the skeletal muscle end plate, they compete with ACh at the receptor, and their effect is reversed by cholinesterase inhibitors. Some drugs in this group may also act directly to close the ion channel operated by the ACh receptor. rocuronium (60–120 s) has the most rapid onset time. Skeletal Muscle Relaxants
Nondepolarizing Neuromuscular Blocking Drugs : Mechanism of Action
1-Succinylcholine is composed of 2 ACh molecules linked end to end. 2- Succinylcholine is metabolized by cholinesterase ( pseudocholinesterase) in the liver and plasma. It has a duration of action of only a few minutes if given as a single dose. 2)Depolarizing Neuromuscular Blocking Drugs: Pharmacokinetics
Mechanism of Action Succinylcholine acts like a nicotinic agonist and depolarizes the neuromuscular end plate The initial depolarization is often accompanied by twitching and fasciculations (prevented by pretreatment with small doses of a nondepolarizing blocker). 2)Depolarizing Neuromuscular Blocking Drugs:
Mechanism of Action Because tension cannot be maintained in skeletal muscle without periodic repolarization and depolarization of the end plate, continuous depolarization results in muscle relaxation and paralysis. When given by continuous infusion, the effect of succinylcholine changes from continuous depolarization (phase I) to gradual repolarization with resistance to depolarization (phase II) (ie, a curare-like block) 2)Depolarizing Neuromuscular Blocking Drugs:
The action of nondepolarizing blockers is readily reversed by increasing the concentration of normal transmitter at the receptors. by administration of cholinesterase inhibitors such as neostigmine or pyridostigmine. In contrast, the paralysis produced by the depolarizing blocker succinylcholine is increased by cholinesterase inhibitors during phase I. During phase II, the block produced by succinylcholine is usually reversible by cholinesterase inhibitors. Reversal of Blockade
1-Respiratory Paralysis:If mechanical ventilation is not provided, the patient will asphyxiate. 2-Autonomic Effects and Histamine Release • Autonomic ganglia are stimulated by succinylcholine and weakly blocked by tubocurarine. • Tubocurarineand mivacurium are the most likely of these agents to cause histamine release, but it may also occur to a slight extent with atracurium and succinylcholine. Toxicity OF NEUROMUSCULAR BLOCKERS
3-Specific Adverse Effects of Succinylcholine A-Muscle pain is a common postoperatively, and muscle damage . B-May cause hyperkalemia, especially in patients with burn or spinal cord injury. C- Increases in intragastric pressure caused by fasciculations →aspiration of gastric contents. Toxicity OF NEUROMUSCULAR BLOCKERS
4-Drug Interactions • A rare interaction of succinylcholine (and possibly tubocurarine) with inhaled anesthetics (isoflurane) can result in malignant hyperthermia. • Aminoglycoside antibiotics and antiarrhythmic drugs may potentiate and prolong the relaxant action of neuromuscular blockers. Toxicity OF NEUROMUSCULAR BLOCKERS
Succinylcholine : ( )A- Has short duration of action (few minutes). ( )B- Can block autonomic ganglia. ( )C- May cause hyperkalemia. ( )D- It’s action can’t reversed by ChEI.s. ( )E- Can cause slight histamine release. Q- Decide wether each stem t or f
Succinylcholine : (T )A- Has short duration of action (few minutes). (F )B- Can block autonomic ganglia. (T )C- May cause hyperkalemia. (F )D- It’s action can’t reversed by ChEI.s. (T )E- Can cause slight histamine release. Q- Decide wether each stem t or f
Clinical uses: 1- Certain Chronic diseases of the CNS (eg, cerebral palsy, multiple sclerosis, stroke) are associated with skeletal muscle painful spasm. 2- Acute injury or inflammation of muscle leads to spasm and pain. B- Spasmolytic Drugs
Drugs for Chronic Spasm Classification: They act in the CNS and in one case in the skeletal muscle cell rather than at the neuromuscular end plate. 1-diazepam, a benzodiazepine. 2-baclofen, a gama -aminobutyric acid (GABAB) agonist. 3-tizanidine, a congener of clonidine. and 4-dantrolene, an agent that acts on the sarcoplasmic reticulum of skeletal muscle. These agents are usually administered by the oral route. B- Spasmolytic Drugs
Drugs for Chronic Spasm • Mechanism of action • Baclofen acts as a GABA B agonist at both presynaptic and postsynaptic receptors, causing membrane hyperpolarization. • Diazepam facilitates GABA-mediated inhibition via its interaction with GABAA receptors. • Tizanidine, has significant α2 agonist activity, reinforces presynaptic inhibition in the spinal cord. B- Spasmolytic Drugs
Dantrolene acts in the skeletal muscle cell to reduce the release of activator calcium from the sarcoplasmic reticulum via interaction with the ryanodine receptor (RyR1) channel. Cardiac and smooth muscle are minimally depressed. • Dantrolene is also effective in the treatment of malignant hyperthermia, a disorder characterized by massive calcium release from the sarcoplasmic reticulum of skeletal muscle. In this emergency condition, dantrolene is given I.V to block calcium release. B- Spasmolytic Drugs
Drugs for Acute Muscle Spasm Eg, cyclobenzaprine, methocarbamol, orphenadrine, are used for the treatment of acute spasm resulting from muscle injury. Most of these drugs are sedatives or act in the brain stem. Cyclobenzaprine, acts by interfering with polysynaptic reflexes that maintain skeletal muscle tone. The drug is active by the oral route. Cyclobenzaprine may cause confusion and visual hallucinations in some patients. None of these drugs used for acute spasm is effective in muscle spasm resulting from cerebral palsy or spinal cord injury. B- Spasmolytic Drugs