Download
1 / 24
240 likes | 257 Views
This case study discusses a neonatal case of Long QT Syndrome with Torsades de Pointes, highlighting the need for innovative treatments and collaboration among multidisciplinary teams. The patient presented with cardiogenic shock and complications like NEC and required various therapies, including Isoproterenol, Magnesium, Propranolol, Mexiletine, Ranolazine, and pacing interventions. The treatment course involved managing multiple episodes of TdP and balancing medication doses to control arrhythmias effectively.

E N D
A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration Melissa Busovsky-McNeal, MD, Frank Cecchin, MD, Meghan Farrell, CPNP-AC, Michelle Ramirez, MD, Puneet Bhatla, MD, Ralph Mosca, MD, and Sujata Chakravarti, MD Congenital Cardiovascular Care Unit 12/12/2014
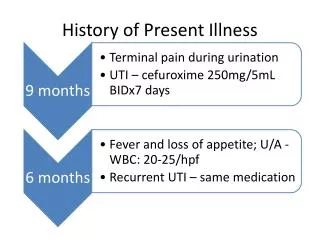
History of Present Illness • A full term female infant was delivered by emergency cesarean section for non-reassuring fetal heart rate • Mother was a gravida one with limited prenatal care • At birth, the patient was noted to be bradycardic with a heart rate of 50-60 beats per minute • An ECG was performed and it demonstrated 2:1 AV block with a corrected QT interval of 620 milliseconds with multiple episodes of TdP • She was treated with IV magnesium and emergently transferred to our institution for further management A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Electrocardiogram on arrival A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Electrocardiogram on arrival A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Hospital Course • On arrival to our institution, she was noticed to be in cardiogenic shock • She developed Multi-Organ Dysfunction Syndrome including: • Acute lung injury • Acute kidney injury • Necrotizing enterocolitis (NEC) requiring exploratory laparotomy • Due to unstable hemodynamics, she was emergently intubated and mechanically ventilated, and inotropic and vasopressor support was initiated • Repeat ECG showed a QTc of 690 milliseconds A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Echocardiography A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Echocardiography A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Echocardiography A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Echocardiography A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Echocardiography A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Hospital Course (cont.) • Due to the inability to administer enteral antiarrhythmics after her episode of NEC, the patient was initiated on IV infusions of Isoproterenol and Magnesium • In spite of these, she continued to have multiple prolonged, but self-terminating episodes of TdP with persistent 2:1 block requiring frequent chest compressions • Once her bowel healed and her gut was tolerating enteral feeds, Propranolol and Mexiletine were initiated A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Hospital Course (cont.) • A trial of Flecainide was also attempted to help control persistent TdP • The patient developed increased frequency of TdP as well as widened QRS complex consistent with Flecainide toxicity • Flecainide was discontinued • At 1 week of age, the patient underwent insertion of a transvenous atrial pacing lead which was externalized to allow for atrial pacing • This resulted in decreased frequency of TdP • Epicardial PM/ICD placement was precluded due to recent laparotomy A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Hospital Course (cont.) • The patient continued to have periods of 2:1 block and TdP in the setting of a persistent, severely prolonged QTc despite improved ventricular function, end organ function and overall clinical status • Ranolazine was added at 4 mg/kg/day • At two weeks of age, the patient underwent LCSD and placement of an epicardial dual chambered PM/ICD. • Weight at this time was 3.28 kg. • Periods of 2:1 block and TdP continued • Three days later Ranolazine was increased to 8 mg/kg/day. A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Hospital Course (cont.) • Subsequently, she was weaned off the Isoproterenol and Magnesium infusions • Due to persistent 2:1 block and periods of Torsades with atrial pacing, the patient’s pacemaker mode was changed to VVI 100 with a hysteresis of 30 • Although her QTc remains prolonged, she now persistently has 1:1 conduction and she has been free of TdP • Studies confirmed the diagnosis of type III LQTS A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Long QT Syndrome Channelopathies A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Genetic Testing • Mutation of SCN5A Presentation TA Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Electrocardiogram A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
QTc Progression During The Hospital Stay A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Echocardiography A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Why Ranolazine? International Journal of Cardiology. 171(1):90-2, Jan 15, 2014 A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
LCSD-Efficacy: Symptom Relief and Sudden Death Protection International Journal of Cardiology. 171(1):90-2, Jan 15, 2014 ~50% symptom free, 10% sudden death in 10 years, 5 to 1 decrease in cardiac events A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Effect of Left Cardiac Sympathetic Denervation on QTc A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
LCSD-Efficacy: Symptom Relief and Sudden Death Protection A Case of Neonatal Long QT Syndrome and Torsades de Pointes Requiring Novel Therapies and Multidisciplinary Collaboration
Thank YouQuestions? Presentation Title Goes Here