Download
1 / 54
890 likes | 3.47k Views
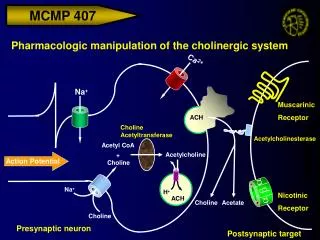
Cardiac action potential. Dr Shreetal R ajan N air. Introduction. Ions Channels/Pores/Carriers & Pumps Channels- Aqueous channel/ Conformational change/ Action usually regulated/ Open to both environment/ Large number of molecules diffuse across

E N D
Cardiac action potential DrShreetalRajanNair
Introduction • Ions • Channels/Pores/Carriers & Pumps • Channels- Aqueous channel/ Conformational change/ Action usually regulated/ Open to both environment/ Large number of molecules diffuse across • Pores- Continuously open to both environment/ No conformational changes/ Always open. • Carriers & Pumps- Not open simultaneously to both environments/ Binding sites/ Limited number of molecules diffuse across Carriers & Pumps maintain the concentration gradients
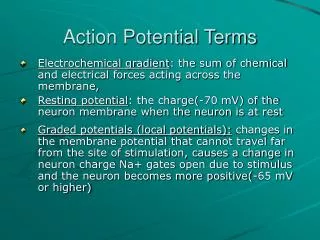
What makes ions to move across? Steady state is reached when the magnitude of the chemical and electric gradients are equal
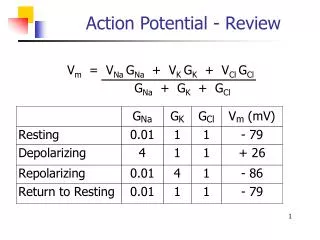
What makes ions to move across? • Nernst equation EK =RT/ZF ln [K]2 / [K]1 Where, • T is temperature [370 C] • R is the gas constant • F is the Faraday constant • Z is the valence of ion [1] • [K]2 and [K]1 are the final concentrations of potassium in compartments 2 and 1, respectively. [150mmol, 5 mmol] • EK is the equilibrium potential for potassium [-90mV] • At equilibrium potential net diffusion is 0 • All ions try to reach equilibrium i.e., tries to drive the membrane potential towards its equilibrium potential • At RMP, membrane is permeable mostly to potassium , hence RMP is close to the EK
Membrane Action Potential • 2 factors • Electromechanical gradient • Open Channels • MAP • Sum of AP generated by different channels [amplitude & direction] • Number of open channels
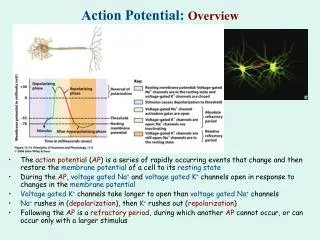
Action potential - definition • Action potential is the net product of mutiple distinctive time and voltage dependent ionic currents. • Complex interaction between depolarising inward currents and hyperpolarising outward currents
ACTION POTENTIAL • Excitable tissues : Neurons Muscles • Action potential duration (APD) Neurons and skeletal muscle cells (1–5 ms) Cardiac myocytes (200-400 ms)
Some terms • Strength of stimulus required to elicit a response or to produce an action potential. • Hyperpolarisation decreases excitability • Small reductions in RMP increase excitability • When RMP is less than the threshold potential the fibre becomes inexcitable Threshold potential- potential at which net inward membrane current becomes large enough to initiate autoregenerative depolarization
Sites of action potential genesis in heart • Nodal tissue – AV node and SA node • His - Purkinje fibres - • Atrial muscle • Ventricular muscle
Refractory period • Refractory Period- - The interval of time during which the cell cannot be re-excited [Absolute RP] - Relative RP • Effective refractory period : minimum interval between 2 propagating AP - Supranormal Excitability
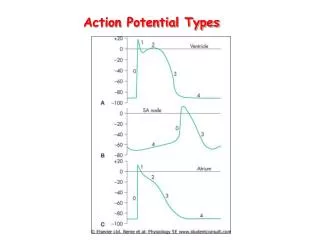
Cardiac AP • Pacemaker potential (slow channel) vs myocyte potential ( fast channel ) • Pacemaker potential occurs in cells capable of producing spontaneous impulses – 1% • Myocyte potential occurs in all other cells – contractile cells – 99%
How a cardiac myocyte is stimulated ? • Spontaneous impulse generation - automatic ( pacemaker) cells • Spread of depolarising current from neighbouring cells ( cardiac syncytium )
Ion channels in the heart • Sodium channels – voltage gated and ligand gated • Potassium channels - voltage gated, inward rectifier and background channels • Calcium channels – transient and long lasting
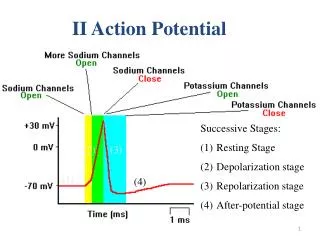
Phase 4 • Represents resting membrane potential • membrane potential when the cell is not stimulated. • this phase will be a horizontal line • caused by the difference in ionic concentrations and conductances across the cell membrane • normal resting membrane potential in the ventricular myocardium is about -85 to -95 mV
Phase 4 • IK1 Current- Membrane stabilizing current [inward rectification • Others-TWIK-1/2 (KCNK1/6), TASK-1 (KCNK3), and TRAAK (KCNK4) • Na/K Pump- 3/2 outward; At fast HR RMP more negative • Low [K]o leads to less IK1 activity, more excitability
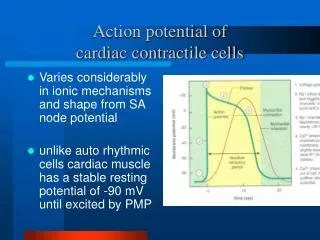
Action potential of a ventricular myocyte and how is it different from action potential of atrialmyocyte • The membrane of the contractile cells remain essentially at rest at about -90mv until excited by electrical activity propagated by the pacemaker cells.
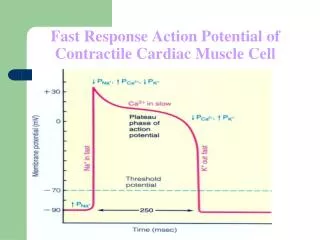
Phase 0 • Rapid depolarisation phase • Opening of the fast Na+ channels causing a rapid increase in the membrane conductance to Na+ • Rate of membrane depolarisation corresponds to conduction velocity
Na+ channels 3 States • Open • Closed • Inactivated • Depends on the RMP
Gating & Inactivation • Closing and opening of channels • Voltage, Metabolic, Stretch
Gating & Inactivation m gate h gate
RMP and Na channels • The slope of phase 0 represents the maximum rate of potential change and is known as dV/dtmax • If the membrane potential is at its baseline (about -85 mV) all fast Na+channels are closed and excitation will open all of them • When membrane potential is less negative some of the fast Na+ channels will be in an inactivated state insensitive to opening • lesser response to excitation of the cell membrane and a lower Vmax
When the resting membrane potential becomes too positive the cell may not be excitable and conduction through the heart may be delayed
SODIUM CHANNEL BLOCKERS • IA – decrease conduction velocity and increase refractoriness • I B – only increase refractoriness • I C - decrease only conduction velocity
Phase 1 • Phase 1 of the myocyte action potential occurs with the inactivation of the fast Na+ channels • The transient net outward current causing the small downward deflection of the action potential is due to the movement of K+ and Cl- ions, carried by the Ito1 and Ito2 currents respectively
Ito currents determine the amplitude and the timing of Ca2+ release from the SR. • In advanced HF Ito currents are downregulated and indirectly affect the Ca currents in phase 2 • Ito currents express differentially at different parts of heart • Maximum in RV, basal region and epicardium • Ito current – ACE inhibitors
Phase 2 • "plateau" phase of the cardiac action potential (absent in pacemaker cells) • sustained by a balance between inward movement of Ca2+ (ICa) through L-type calcium channels and outward movement of K+ through the slow delayed rectifier potassium channels - IKs
Phase 3 • L-type Ca2+ channels close • slow delayed rectifier (IKs) K+ channels are still open. • more types of K+ channels open.- Ikr,Ikur,Ik1 • the rapid delayed rectifier K+ channels (IKr) • inwardly rectifying K+ current, IK1 • Additional channel in atrial muscle ( I kur ) • Vernakalant has action on this channel RESULT IN REPOLARISATION
Refractory period - explanation • Absolute refractory period - Sodium channels are in an inactivated state - • Relative refractory period - sufficient number of sodium channels have transitioned back to their resting state – a stronger stimulus can generate AP
Refractory period • Absolute refractory period - beginning of phase 0 until nearly the end of phase 2 • Relative refractory period - phase 3 and phase 4 - caused by changes in the state of sodium and potassium channel molecules
Afterdepolarisations • Positive potentials that occur during the repolarisation phase of the action potential Types : • Early – phase 2 and phase 3 • Delayed – phase 4 • Important in the genesis of arrhythmias
Action Potential of the pacemaker cells • The pacemaker cells do not have a stable resting membrane potential like the nerve and the skeletal muscles. • Instead they have an unstable membrane potential that starts at – 60mv and slowly drifts upwards towards threshold. • Because the membrane potential never rests at a constant value, it is called a Pacemaker Potential rather than a resting membrane potential. • Phase 1 and 2 typically absent.
IONIC BASIS OF ACTION POTENTIAL OF PACEMAKER CELLS Phase 4: Pacemaker Potential: Opening of voltage-gated Sodium channels called Funny channels (If or f channels ). Closure of voltage-gated Potassium channels. Opening of Voltage-gated Transient-type Calcium (T-type Ca2+ channels) channels . Phase 0: The Rising Phase or Depolarization: Opening of Long-lasting voltage-gated Calcium channels (L-type Ca2+ channels). Large influx of Calcium. Phase 3: The Falling Phase or Repolarization: Opening of voltage-gated Potassium channels Closing of L-type Ca channels. Potassium Efflux.
Phase 4 • Diastolic depolarisation • Chronotropism or the rate of heart beat depends on the slope of pacemaker potential • modulation by the autonomic system of the cardiac SAN rate also takes place in this phase • Sympathetic stimuli induce the acceleration of rate by increasing the slope of the pacemaker phase • Parasympathetic stimuli has opposite effect
Regulation by autonomic nervous system • Parasympathetic activation - c AMP levels decrease and open additional K channels and produce more hyperpolarisation. • - phase 4 takes longer to reach the threshold voltage • Sympathetic activation - increase c AMP levels and this in turn open calcium channels
Autonomic nervous system modulates the frequency of depolarization of pacemaker
Refractory period • In fast channels ERP/APD < 1 : Na channels recover in a voltage dependent manner above the threshold potential • In slow channels ERP/APD > 1 : Ca channels recover only in a time dependent manner progressively after the fiber has fully repolarised