Download
1 / 25
250 likes | 445 Views
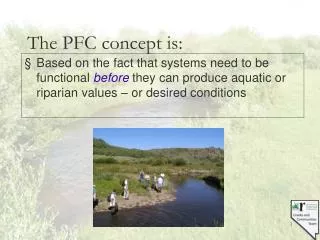
PFC Medical Planning. Use the 10 Capabilities Grid to Figure out what capability you are deficient on and then Identify what asset in your AO has it available. Couldn’t get a ventilator to bring? Make finding one a priority in your planning and note it on your grid and map.

E N D
Use the 10 Capabilities Grid to Figure out what capability you are deficient on and then Identify what asset in your AO has it available. • Couldn’t get a ventilator to bring? • Make finding one a priority in your planning and note it on your grid and map
Add Regional Map And Locations Clinic Team Houses / Bases 600km LZ 143 C-130 Coalition Med Facility / Team Host Nation Med Facility Air Port / Landing Strip H LZ / FARP MSS 600km Range / Distance Scale
Add Local Map and Locations Clinic Team Houses / Bases 50 km H Coalition Med Facility / Team LZ 143 MI 17 Helo Host Nation Med Facility Air Port / Landing Strip H LZ / FARP MSS 50km Range / Distance Scale
Medical/CASEVAC CONOP slide • Why • Amount of force providers rotating • Different medical plans • Lack of research • Mutual support • Other COCOM priorities • Squeezing the balloon
Header/top of slide Classification noted Country of operations. If it’s multiple countries, use SOCFWD flag SOCAFRICA flag on the right Title will be Operation/Team name MEDEVAC or CASEVAC CONOP
Medical Capabilities Focus to care is beyond the capabilities of SF/SOF medic “Self aid/buddy aid” and “all team members are TCCC qualified” are unacceptable- already assumed. Underwear goes on the inside. Designated numbers/letters within this block will correspond throughout the plan. Triangle will correspond with the medical risk scale at the bottom and the map The circled numbers will correspond where on the map they are located
CASEVAC PLATFORM: Thought should be given to infil and exfil platform. Can they loiter if immediate exfil is needed? Include all platforms intended to be used in CASEVAC plan (Contract Aviation, Personal Recovery, SOCAF owned, Coalition and HN (if feasible). What is your platform’s spin up and launch times over the geographical distance?, Thought to platforms ability to land on improved/ unimproved surfaces and travel time and speed. This needs to be captured in a narrative portion of the plan and depicted on the map to the right.
PACE OPTIONS A coherent application of assets available to you
Considerations & Limitations Highlight relevant issues not noted “Driving through Nairobi at night will affect patient transportation to AGA KHAN “Pilots are not NVG qualified to fly at night” Relevant facts to this specific mission What are the refuel times if you have to “lily pad” across to your next destination? What are your patient transfer times? Expect changes due to operational needs
Medical Risk Scale This is in reference to your BEST plan; which is your “P.” “ER” is your primary ER “DCS” is your primary DCS Definitions: ER – Emergency Room is a facility/location that is able to stabilize a patient prior to surgery. It’s also a capability above the tactical element (ex: TCCET, MOG UN ER, CCET, SOST) DCS- Damage Control Surgery is the rapid initial control of hemorrhage and contamination with packing and a temporary closure.
MAP This is a pictorial representation of all the information we had on the left translated onto the map A visual for your information Should systematically match what you have on the left The Blue triangles connote where your closets American DCS and ER assets are located and matches your medical risk scale
CONTACT INFORMATION Order of precedence of phone numbers Clear and concise Split up in 2 sections: Internal/External Internal should be “down and in” External should be “up and out” Phone numbers should be limited due to the SOCFWD JOC’s and the Surgeons will coordinate follow on care.