Download
1 / 33
330 likes | 373 Views
Lumbar Spinal Stenosis Decompression. Prof. Dr. R. Kemal Koç Department of Neurosurgery Erciyes University , Faculty of Medicine Kayseri , Turkey. Degenerative lumbar spinal stenosis. S lowly progressive spinal disease common in the elderly population LF hypertrophy,

E N D
Lumbar Spinal StenosisDecompression Prof. Dr. R. Kemal Koç Department of Neurosurgery Erciyes University, Faculty of Medicine Kayseri, Turkey
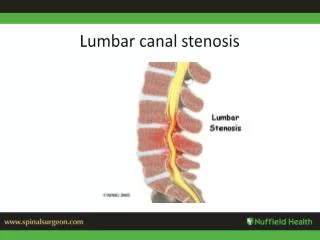
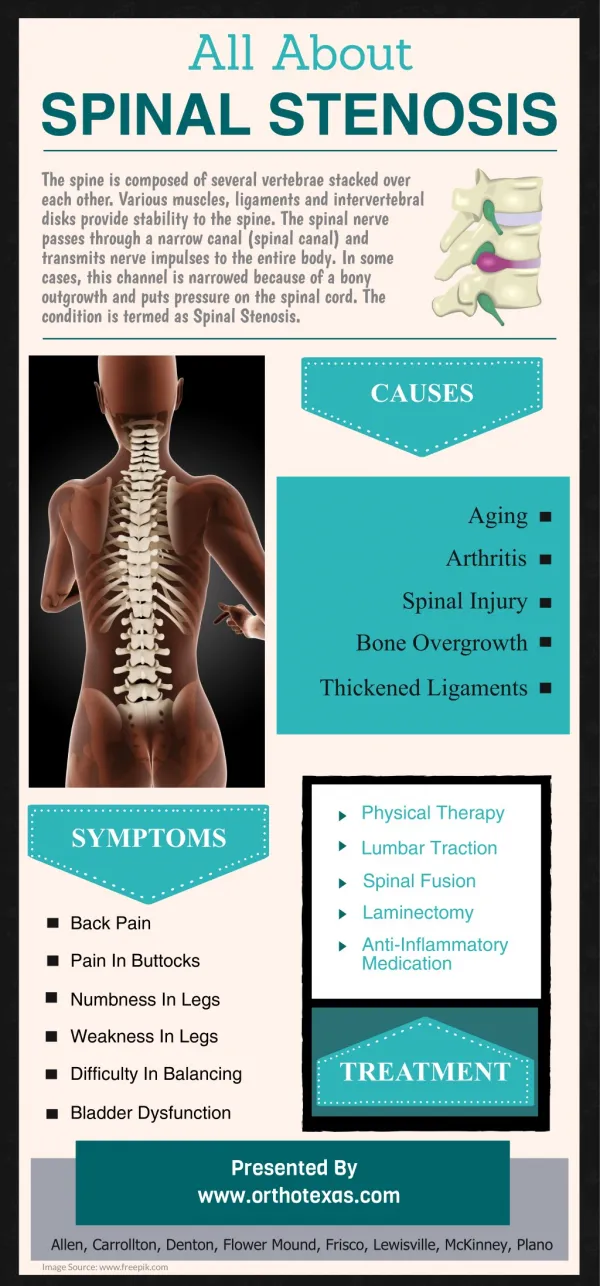
Degenerative lumbar spinal stenosis • Slowly progressivespinal disease common in the elderlypopulation • LF hypertrophy, • Facet joint thickeningwitharthropathy • Bulging of the intervertebral disc • Eventually leading to compression ofthe neural elements
Indications for surgery • Neurogenic claudicationor radiculopathy • Failure of conservative treatment • nonsteroidal antiinflammatory drugs • corticosteroids • physiotherapy • Patient selection criteria • CT or MR imaging evidence of lumbar degenerative stenosis
Surgical technique for DLS • The chosentechniqueinherently depends on the stability of the DLS. • The following preoperative parameters are predictors of stability in DLS • the absence of low-back pain, • no facet joint effusions on MR, • restabilization signs (disc heightloss, osteophyte formation, vertebral endplate sclerosis, and ligament ossification), • no disc angle change or less than 3mm of translation on dynamic radiographs. • Decompression alone is sufficient in the stable cases Simmonds AM. Defining the inherent stability of degenerativespondylolisthesis: a systematic review. J Neurosurg Spine 23:178–189, 2015
Positioning for surgery • The patient is placed prone in marked flexion (lumbar hyperflexion position or knee–chest position ) • Opens the spinal canal and facilitates dissection, while freeing the abdomen and limiting blood loss • Intraoperative X-Ray films • A lateral confirmatory film is routinely used
Exposure • After placing of a Williams retractor, the procedure is performed microsurgically. • Care is taken not to injure the facet capsules as the muscles are retracted laterally.
Basic principles of decompression technique • Theintraoperativecomplication of an incidentaldurotomy can be markedlydecreased • Thinning of thelaminaandhypertrophic bone with a high-speedburr • Theuse of a blunt dissector or nerve hook toreleaseadhesions • A smallpunchusedtoremovethelastlittlepieces of bone • Performingthedecompression in caudaltocephaladdirection • The usage of microscope and microsurgery tool.
Basic principles of decompression technique • Spinal stability should be protected during decompression • More than 50% of the facet joints should not be removed. • Nerve root can be decompressed by removal of the medial 1/3 of superior articular process. • Pars interarticularis should be protected at least 5 mm wide. • Dissector must be easily moved throughout the course of decompressed nerve root after decompression
Laminectomy Hemilaminectomy/hemilaminotomy Bilateral hemilaminotomy Hemilaminotomy and bilateral decompression Trumpet laminectomy Expansive laminoplasty Microendoscopic posterior decompression Decompression
Laminectomy • Traditional surgeryis wide laminectomy, whichallows decompression of the neural structures by unroofingthe spinal canal. • The success rate of this procedurevaries from 62 to 70%, • Frequent surgical failuresare generally related to postoperative iatrogenic spinalinstability. Airaksinen O, Spine 22:2278–2282, 1997 Javid MJ,J Neurosurg 89:1–7, 1998 Silvers HR, J Neurosurg 78:695–701, 1993 Turner JA, Spine 17:1–8,1992
Hemilaminotomy and bilateral decompression • The ipsilateral lamina is partially removed, and the base of the spinous process is undercut • By medial angulation of the microscope, the contralateral lamina is partially removed • The ipsilateral and contralateral ligamentum flavum is resected • Decompression of the ipsilateral and contralateral resess is achieved by undercutting the medial part of the facet Spetzger U. Acta Neurochir (Wien). 1997
Hemilaminotomy and bilateral decompression Advantages • Spinal instability is minimal • Spinous process, interspinous and supraspinous lig are preserved • Contra-lateral paravertebral muscle is preserved • Less blood loss • Short hospitalization period • Better results • 80% good or excellent result • 97% patient satisfaction • It is alsousedformultilevelstenosis Disadvantages • Restenosismayoccur Costa F, J Neurosurg Spine 7(6):579-86, 2007 Morgalla MH, J Neurosurg Spine 14:305-312, 2011 Thomé C, J Neurosurg Spine 3(2):129-41, 2005
Hemilaminotomy and bilateral decompression in degenerative spondylolisthesis • The presence of Grade I spondylolisthesis without segmentalinstability was not considered a contraindication to this surgical approach. • Better results are reported in the cases with hemilaminotomy and bilateral decompression in degenerative spondylolisthesis, although the slippage progressed. Sasai K. J Neurosurg Spine 9:554–559, 2008
Hemilaminotomy and bilateral decompression in degenerative spondylolisthesis • A larger facet effusion size (1.3±0.9) in the patients with lumbar degenerative spondylolisthesis strongly suggested that the affected segment had been instabilized. • If interfacet space is separated and T2 hyperintense, only canal decompression is insufficiency, instrumentation should be added. Hasegawa K, J Neurosurg Spine 12:687–693, 2010 Oishi Y,J Neurosurg Spine12(1):88-95, 2010
Case: 52-year-old woman presents with a 3-year history of low back pain, Neurogenic claudication 50 m +
Case: 53 years old, female: neurogenic claudication 50 m + for 3 years, low back pain for 10 years. PO 5. months; walking normal, mild lowback pain.
Case:SS 70 years old, male, neurogenic claudication 100 m, low back pain for 3 years
Recurrence of stenosis after surgery • No regrowth 12% • Mild regrowth 48% • Moderate regrowth 28% • Marked regrowth 12% • Of the patients with marked regrowth, 60% had a unsatisfactory clinical result Postacchini F, J Bone Joint Surg, 1992
Indications of instrumentation • Instability • Progressive deformity (scoliosis, kyphosis) • Resection of more than 50% of facet • Extensive decompression with an underlying deformity • Significant loss of lordosis • Stenosis develops at a previously decompressed segment
Complications • Dural tear • Cauda equina syndrome • Nerve root injury • Epidural hematoma • Infection Delayed complications • Segmental instability • Epidural scar formation
CONCLUSION • Microsurgical bilateral decompression via unilateral approach is a useful and safe operative procedure for LSS patients. • Sufficient clinical results is obtained even in the patients with multiple-level LSS, if the patient is correctly selected and the microsurgical decompression surgery is carefully performed.
Type of stenosis 1) Purely hypertrophic changes of the LF 2) Marked hypertrophic bone spurs arising from thefacet joints 3) Combined arising from LF hypertrophyand/or calcification and osteophytic spurs
Clinical presentation • Bilateral neurogenicclaudication • Intermittent pain radiating to the thighand/or leg, which is • aggravated by prolonged standing orlumbar extension • relieved by sitting or flexing the lumbarspine • Radicular deficits are sometimes present
Prognosis • Many variables (due to type of stenosis, number of stenosis, applied surgical method, etc.). • Overall, good or excellent result is 82%. • Good or excellent result is 96% in non-related symptoms with posture. • Low back pain is more likely to continue after the decompression. Granz JC. J Neurosurg 72:71-74, 1990
The crucial technical steps are as follows. • The superiorlamina (exceeding the midline of the attachment of thespinous process by ~3 mm) and medial portion of facet joint are partiallythinned using a microdrill. • The Kerrison tipshould be forced beneath the lamina, starting from the midlinewhere the LF attachment is very loose. F. Costa J Neurosurg Spine 7:579–586, 2007
The crucial technical steps are as follows. 3) The laminarthinning should be performed, leaving the LF beneath intactto protect the dural sac. 4) Bone thinning should beextended until the upper border of the LF and the dural sacare visible.
5) The LF is elevated using dissectors and biopsyforceps, thus creating a neat cleavage plane with thedural layer before any dissection is attempted.
6)At this point, with the dural layer clearly in view, bone andthe LF are removed in a standard fashion, reaching the midlineand decompressing the ipsilateral radicular recess • The nerve root is decompressed by undercutting the medial third of the superior articular facet • After the decompression, a dural elevator should be able to pass along the course of the nerve root without any impedance
7) Finally, the operating table is elevated, and the operativemicroscope is gradually tilted toward the oppositeside at the proper angle, thus allowing as much of the contralateralLF as possible to be removed using the smallKerrison rongeurs.
8) The base of the spinous process can befurther drilled, and the inner portion of the facet joint canbe undercut until the contralateral spinal nerve root anddural border can be seen.
9) If necessary, a contralateral foraminotomycan be performed.because the spinal root canbe easily identified (Fig. 1D).
10) Obviously, in cases oftight adhesions, some small pieces of the LF can be left inplace.