Download
1 / 63
640 likes | 782 Views
“Opening the Mouth” Continuing MCH Education in Oral Health. Columbia University School of Dental and Oral Surgery Division of Community Health. Learning Objectives. Understand the connection between oral health and overall health

E N D
“Opening the Mouth”Continuing MCH Education in Oral Health Columbia University School of Dental and Oral Surgery Division of Community Health
Learning Objectives • Understand the connection between oral health and overall health • Understand that dental caries is an infectious, transmissible, communicable disease • Understand the prevalence, acuity and consequence of dental disease • Understand dental care finance, delivery and workforce issues • Be able to list general action steps that can be taken to decrease oral health disparities • Describe action steps specific to Title V Maternal and Child Health Federal Block Grant programs that can be taken to decrease oral health disparities
Oral Health and Health Care Introduction: Despite great strides in improving oral health, disparities still exist across all population groups. Those suffering the worst oral health are the poor of all ages, particularly children and older Americans. Racial and ethnic minority groups also experience a disproportionate level of oral health problems. Medically compromised individuals or those with disabilities, are at an increased risk for oral diseases, which in turn, further jeopardizes their overall health (1). Tooth decay remains the single most common, chronic disease of childhood; 5x more prevalent than asthma (1). Children suffering the highest rates and most severe dental disease tend to be preschool-aged and disadvantaged by poverty, minority status or social conditions. Approximately 25% of children under age 19, account for 80% of the dental disease. Dental disease, untreated, results in pain, and infection, and may inhibit general growth and development (2).
Oral Health and Health Care Periodontal disease and chronic oral infections are considered a risk factor for heart disease, inadequate glycemic control in diabetics and more recently, poor pregnancy and birth outcomes. “Oral diseases and conditions may have a significant impact on general health…..Oral health care is an important, but often neglected, component of total health care. Regular dental visits provide an opportunity for the early diagnosis, prevention, and treatment of oral and craniofacial diseases and conditions for persons of all ages, as well as for the assessment of self-care practices”. (3) To help reduce oral health disparities, there needs to be an increased understanding and awareness among the community, health care providers, and policy makers at the local state and federal level. Oral health must be integrated into overall health, and barriers to care need to be eliminated.
Part I: Conception to Birth • Meet Mrs. Perez. She is a 32-year-old, Hispanic mother of 2 children, under the age of 6 years, and pregnant for her third. • She presents to the dental clinic at her local community health care center, complaining of “bleeding gums and loose teeth”. • Her dental pain has progressed to the point that eating has become difficult. • Mrs. Perez was unable to attend the clinic prior to today, as she could not afford to pay for the dental treatment, not to mention child-care for her 2 children and the cost for public transportation. • The private dentist located “relatively” close to her inner-city home, informed her that he “does not accept Medicaid”. • After her examination, the dentist informs Mrs. Perez that she has periodontal or “gum” disease.
Periodontal Disease • The case of Mrs. Perez is unfortunate, but commonplace in community health center dental clinics. • The reality of this case? • Hispanic and African American populations have higher rates of oral disease and tooth loss than the white, non-Hispanic majority population • Approximately 26% of adults aged 18-34 years, do not have health insurance (1) • 72% of adults not obtaining dental care state that the major reason is financial (4) • Few dentists participate in the Medicaid program (approx 1/3 of dentists provide at least one dental appt under medicaid, & only 14% are active medicaid providers, i.e.. billing > $10,000 as a percentage of total active patients) (5) • There is a decline in the number of dentists per 100,000 people and it is anticipated this shortage will increase over time. As of June 2003, 2112 dental health professional shortage areas have been identified. It would take 8481 additional dentists to achieve a target dentist-to-population ratio of 1:3,000. (6)
Periodontal Disease • The number of underrepresented minorities in the dental profession is significantly low compared to their proportion in the overall population (5.7% of graduate dentists are African American and 5.3% are Hispanic; These percentages are far below the percentage of African American (12%) and Hispanics (11%) in the general population) (7). Thus, patients may be faced with language barriers and/or cultural incompetence. • Safety net facilities (e.g. dental schools, community health centers, hospital clinics and mobile vans) are few in number compared to the medical safety net (primarily because community hospital emergency rooms comprise a major component of the medical safety net, whereas emergency rooms typically only offer palliation with medication for dental complaints. In addition, there are 4x as many medical schools than dental schools. • Although only 1% of Medicaid expenditures is related to dentistry (0.5% for children)(8), fiscal demands have led to reductions in, or elimination of dental benefits for adults and the disabled. In 2003, only 8 States had comprehensive adult dental coverage under Medicaid, while 43 States had no coverage or limited coverage (53)
Despite pain and discomfort, some women never present for care (Fact: less than two thirds of adults reported having a dental visit in the last year{1}). What happens if Mrs. Perez does not receive the necessary dental treatment for her periodontal disease? The most obvious consequence will be continued mouth pain, disease progression and eventual tooth loss. But what about the systemic effects of her periodontal disease? How will her oral disease affect her pregnancy or her unborn child? Learning Objectives: What is the association between periodontal disease and poor birth outcomes What is the putative biologic pathway What is the effectiveness & evidence for intervention Periodontal Disease:Poor Birth Outcomes
Periodontal Disease:Poor Birth Outcomes Periodontal Disease: • Periodontal disease (periodontitis or “gum disease”) is a chronic infection caused by bacteria existing at the gum line in the form of plaque and calculus (“tarter”). (Picture of periodontitis – Papos Papapanou- waiting for picture) • Periodontal disease causes inflammation and bleeding gums and, if not treated, leads to tissue destruction, tooth mobility and eventually tooth loss. • Growing body of research supports an association between periodontal disease and Pre-term low birth-weight (PLBW) (link to studies further on in module)
Periodontal Disease:Poor Birth Outcomes Preterm Low Birth-weight: • PLBW pregnancy outcomes in the U.S. remain a concern because of the significant consequences to maternal and child health, high costs, long-term disease burden, and individual suffering. • Economic consequences exceed $5 billion annually • Accounts for 6-9 percent of all births (9) • Centers for Disease Control maintains that the second leading cause of infant mortality is premature/low birth-weight (10) • Accounts for 70% of all perinatal deaths and 50% of long-term neurologic morbidity (9) • NIH reports that “as many as 18% of the 250,000 premature low-weight infants born in the United States each year may be attributed to infectious oral disease” (call out box?)(11)
Periodontal Disease:Poor Birth Outcomes State of the Science: • Known causes of PLBW, that may be medically managed, include asthma, cigarette smoking, bacterial vaginosis and diabetes • However, much of its incidence remains unexplained • Classic measures for association between periodontal disease and poor birth outcomes, are being explored and show likely causality • Based on this emerging science, there is hope that the severe developmental, behavioural, health and economic consequences of PLBW may be minimized by improving oral health during pregnancy
Periodontal Disease:Poor Birth Outcomes State of the Science: • Animal Studies • Inducing experimental periodontitis in animals, leads to significantly smaller litter weights (12). • These animals show higher levels of blood-borne chemical mediators that are responsible for causing uterine contraction, cervical dilation, labour and abortion (13).
Periodontal Disease:Poor Birth Outcomes State of the Science: • Humans studies: • The association was first identified by secondary analysis of NHANES III (13) • One case-controlled study, after adjusting for all other risk factors (e.g. tobacco use and maternal age) found that women with periodontal disease had 7 times the risk of delivering a PLBW baby (13). • More recent human studies following women through pregnancy, compares favourable and unfavourable birth outcomes. Preliminary results indicate that mothers with advanced periodontitis have a higher risk of delivering a PLBW infant. (14,15) • NIH supported, multicenter, RCT studies are currently underway
Periodontal Disease:Poor Birth Outcomes Effectiveness and Evidence for Intervention: • Can treating periodontal disease in pregnancy reduce poor birth outcomes? • Two studies have shown an association between treating periodontal disease during pregnancy and improved birth outcomes (16, 17) • For the mother, there are no known negative consequences associated with improving the oral health of pregnant women. The positive is that it may reduce poor birth outcomes, which is a considerable benefit for the child. Thus, there is great enthusiasm in promoting optimal oral health during pregnancy.
Dental Care for Pregnant Women The National Healthy Mothers, Healthy Babies Coalition (HMHB): • Issued a statement of position that “oral health care during pregnancy is crucial and should be available to all women, regardless of income level”. They are committed to “working with dental and other health care providers to increase awareness of, and support research on, the possible link between periodontal disease and pre-term, low birth-weight babies” (18) • See The National Healthy Mothers, Healthy Babies Coalition Position Statement on Oral Health and Pregnancy at www.Hmbh.org/ps_oral health.html American Academy of Periodontology: • Has recently developed a draft policy statement that recommends pregnant women have a periodontal examination performed and appropriate preventive and/or therapeutic services provided, as there is immerging evidence that women with periodontal disease may be more at risk to deliver a preterm low birth weight baby (August 2003) • See the AAP website @ www.perio.org
Dental Care for Pregnant Women • Clinical guidelines suggest that routine plaque and calculus removal via polishing, scaling and curettage, can be performed safely during pregnancy, regardless of trimester (19). • Dentists and obstetricians agree that routine dental care should be maintained throughout pregnancy. (20,21) • Despite the growing evidence and literature to support the association between periodontal disease and PLBW, it has not been widely translated into clinical or public policies.
Medicaid programs, administered by the states within federal guidelines, are required to provide certain populations with specified (“mandatory”) benefits. Dental is only mandated under Early and Periodic, Screening, Diagnostic, and Treatment Services Program ( EPSDT). Dental coverage for pregnant women (+ 21 years) currently is not a “mandatory” benefit (see note) Pregnant young women (< 21 years) that are covered by Medicaid, must be enrolled under the EPSDT to receive comprehensive dental benefits (22) Centers for Medicare and Medicaid Services (HCFA) Medicaid Services State by State, October 1, 1996. HCFA Publication 02155-97. California: first in the nation to extend dental benefits to pregnant women Adult women and minors who are pregnant become eligible for either adult dental coverage (if over the age of 21) which includes periodontal treatment or the full range of EPSDT dental services, which also include periodontal treatment (23) Note: Louisiana and Utah have recently added benefits – Waiting for info from Ann DeBiasi at CDHP (Insert this in a “popup” box ?) Oral Health Programs for Pregnant Women
Oral Health Programs for Pregnant Women • In California, with the addition of preventive periodontal to the scope of Medi-Cal benefits for women in the pregnancy services only and pregnancy and emergency services only aid categories, the estimated savings for fiscal year 2004-2005 is $24,427,000 (23). • (Based on the estimate that in FY 2003-2004, the number of Medi-Cal low birth-weight babies attributable to periodontal disease is estimated at 2,655. The average neonatal savings per child is $22,000. Approx. 50% of women will complete sufficient preventive periodontal care to bear a normal birth-weight infant
Mrs. Perez was unable to undergo periodontal treatment as she could not afford to pay for the service. Six months after her visit to the health center dental clinic, she delivers a preterm low birth-weight baby girl, named Maria. • Fortunately, with advances in neonatal care, survival rates of pre-term, low-birth-weight babies have dramatically improved. • Unfortunately, studies indicate that pre-term children suffer from a multitude of acute and long-term problems, including significant delays in physical and psychological growth and development of all structures, including the craniofacial complex and teeth • Oral structures, like other tissues, are affected by prematurity and low birth- weight (24)
Part II: Early Childhood Tooth Decay Learning Objectives: • Understand the goal of early intervention and importance of the “dental home” • Define dental caries (tooth decay) • Differentiate between dental caries and early childhood tooth decay • Describe the transmission and colonization of bacteria associated with early childhood tooth decay • Understand the prevalence and consequence of early childhood tooth decay • Describe conventional treatment (restorative dentistry) • Describe emerging treatment (Prevention and disease management)
Early Childhood Tooth Decay • Now meet 12 month-old Maria Perez. • During Maria’s well-baby exam at her primary care physician’s office, Mrs. Perez states that Maria’s front teeth “didn’t look right” when they erupted. The health history indicates that Maria was a pre-term infant (i.e.. < 37 weeks gestation) with a low birth weight (i.e.. < 2500gm). • Her physician takes a brief look, reassures Mrs. Perez that it may be a “developmental problem” and suggests if she has further dental concerns, that she should see a dentist. He does not write a referral letter.
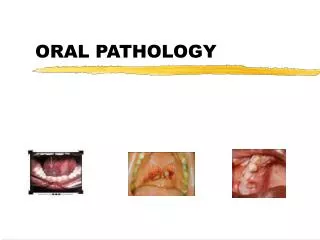
Early Childhood Tooth Decay • As young as Maria is, both developmental and acquired disease are already evident on examination. Active Disease: • Maria was noted to have thick plaque and decalcification (mineral loss) on her primary teeth (red arrow). The gingival tissue appeared shiny and full (blue arrow), indicating inflammation. Developmental Findings: • Notching of incisors (yellow arrows), eruption hematoma (purple arrow), atypical eruption sequence (pink arrow), and an anatomical variant of the labial frenum (green arrow)
Early Childhood Tooth Decay • What is the most important clinical finding during Maria’s oral exam? • It is the abundant plaque on her front teeth. • Visible plaque on the front teeth, is positively correlated with caries development by age 3 (28)(Call out box?) • The primary components of dental plaque are bacteria. Acid, produced by these bacterial species (mainly Streptococcus mutans) is considered the most important activity in the production of tooth decay. • Maria,being a low birth-weight infant, is at risk for enamel hypoplasia, as 20% of low birth-weight children are affected. • Enamel hypoplasia is defined as a deficiency in enamel formation, that manifests clinically as grooves or pits, or a lack of surface enamel (29). These surface irregularities act as “plaque traps” allow for an increased colonization of harmful bacteria and increase Maria’s risk for developing cavities.
Early Childhood Tooth Decay • Why should Maria’s physician refer her to a dentist? • The goal of an early dental assessment is primary prevention (see slide 36). This may be accomplished with the timely delivery of oral health information, including the conditions that create caries & cavities; its natural progression; and its prevention (Anticipatory Guidance – see slide 37), and the identification of populations at high risk for tooth decay, • The traditional approach of treating the effects of tooth decay (i.e.. “drilling and filling”) is being replaced by disease prevention and disease management. • Prevention focuses on the establishment and maintenance of good oral hygiene,optimizing systemic and topical fluoride exposure, and eliminatingprolonged exposure to simple sugars in the diet. Prevention is the foundation for the establishment of a “dental home” by 1 year of age. • The concept of the "dental home" is derived from the AmericanAcademy of Pediatrics concept of the "medical home." This concept states that “the primary health care of infants,children, and adolescents should be accessible, continuous,comprehensive, family centered, coordinated, compassionate,and culturally effective. It should be delivered or directedby well-trained child health specialists who provide primary care and helpto manage and facilitate essentially all aspects of pediatriccare” (25).
Early Childhood Tooth Decay • Advances in the understanding of dietary influences and fluoride on dental disease become instrumental in supporting early intervention • Every child should have an examination and oral health risk assessmentby 12 months of age by a dentist or qualified pediatric health care professional. (26) • The Caries Risk AssessmentTool (CAT), provided by the American Academyof Pediatric Dentistry (27), was designed to assist both dental and nondental health professionals in assessing the risk of tooth decay in infants, children and adolescents. • The CAT can be used to determine the relative risk of caries of thepatient • Questions directedat dietary practices, fluoride exposure, oral hygiene, utilizationof dental services, socioeconomic status and general level of health can help determine if a child is at low, moderate or high risk for dental disease. • Using the CAT ( http://www.aapd.org/members/referencemanual/pdfs/02-03/Caries%20Risk%20Assess.pdf ), and Maria’s history (low socioeconomic status and no usual source of dental care) and exam findings (thick plaque, areas of demineralization and gingivitis), Maria would be considered at high risk for dental disease.
Early Childhood Tooth Decay • It is too late for Maria to gain the advantage of primary prevention and some aspects of anticipatory guidance, as she already exhibits signs of dental disease. • Maria is not too late for disease suppression (see slide 39). With proper diet control and the application of topical fluoride, Maria may have avoided surgical intervention. Unfortunately, without a timely dental referral, disease progression is inevitable. • The referral was never made from Maria’s physician to a dentist and Mrs. Perez fails to seek care on her own.
Early Childhood Tooth Decay • Maria is now 33 months old. • She has presented with her mother to the local health center dental clinic, because, according to Mrs. Perez, Maria has “been up all night, crying about her teeth”. • Dental History- in the last 2 months, Maria has become increasingly irritable at mealtimes. It began as whining with cold or sweet foods, and has progressed to crying when biting with the front teeth. For the last 3 nights Maria has awoken from sleep and Mrs. Perez was able to console her with her usual bottle of apple juice. • Last night, she was inconsolable and required pain medicine (“oral numbing gel”) to help her sleep. • Mrs. Perez did not take Maria to the dentist before, as her local dentist doesn’t except medicaid and she is aware of the unpredictable wait and long hours for walk-in “emergencies” at the health center. Additionally, Mrs. Perez stated that her physician said it was a “developmental problem” and she felt since these are “baby teeth”, that they will “just fall out, so why bother fixing them”. Maria’s upper (maxillary) teeth, with severe early childhood tooth decay
Early Childhood Tooth Decay Failure of Early Intervention? Tooth decay in the primary teeth, has significant functional and disease progression consequences: Disease • Since the mouth is the locus of disease, and not all the primary teeth are replaced simultaneously, disease in the primary teeth will spread to the incoming permanent teeth. Dental disease impacts all the new teeth as they become available, and because the exchange takes so long (12-13 years), children that have untreated, active oral disease are at an increased risk for more generalized, severe tooth decay. Child • As can be seen in Maria’s case, early childhood tooth decay in the primary teeth, if not cared for, results in chronic pain, infection and sleepless nights. It may also lead to poor weight gain, the inability to eat (2) and affects overall quality of life. (30) Dentition • Loss of primary teeth impairs mastication, affects the development of the craniofacial system, and results in loss of arch space for the succeeding permanent teeth to “grow in” (erupt) into the proper position.
Early Childhood Tooth Decay • Maria is diagnosed with severe early childhood caries or “tooth decay”. Maria’s upper (maxillary) teeth, with severe early childhood tooth decay
What is dental caries? Dental caries, better known as “tooth decay”, is the disease process that leads to the loss of tooth mineral and eventually, cavitation of the tooth surface (“cavity”). It is a dieto-bacterial, infectious, transmissible, oral disease. Three things are required for dental caries activity to become established: one or more susceptible tooth surfaces, "cariogenic“ (decay causing) bacteria and fermentable carbohydrates (particularly sucrose). What is early childhood caries? Early childhood caries (ECC) or early childhood tooth decay, previously termed “nursing caries” or “baby-bottle tooth decay”, is a particularly virulent form of tooth decay, that affects the teeth of infants and preschool children. It resultsfrom an overgrowth of specific organisms that are a part ofdental plaque (sticky white or yellow film found on the tooth surface) . Although numerous types of bacteria live in the mouth, tooth decay results from the overgrowth of specific cariogenic (decay causing) organisms. Studies demonstrate that children with early childhood tooth decay, have Streptococcus mutans (S. mutans),counts that exceed 30% of the cultivable plaque flora (31-33). Conversly, in children with negligible to no caries activity, S. mutans comprises less than 1% of total cultivable flora (34). Thus, S. mutans have been implicated as the most likely infectious etiologic agents of tooth decay (35). Early Childhood Tooth Decay
Early Childhood Tooth Decay Transmission and Colonization: • Infants are colonized with the eruption of the primarydentition at approximately 6 to 30 months of age. The primary caregiver of the infant, frequently the mother, has been shown to be the most likelysource of inoculation of an infant’s dental flora. There are no studies that explain absolutely how transmission occurs, however, examples include cleaning the baby's pacifier in the mother's mouth before giving it to the baby, sharing utensils or pre-chewing the baby's food. • Transmission and colonization of S mutans depends on the magnitude of the innoculum. Higher levels of S mutans are associated with untreated tooth decay, thus, infants of mothers with untreated tooth decay are at higher risk of acquiring the bacteria (36)
Early Childhood Tooth Decay Acid Production and Demineralization: • Decay causing bacteria ingest sugar and other fermentable carbohydrates and produce acid as a by-product, causing a drop in the plaque pH. The acid attacks the outer surface of the tooth (enamel) for approximately 20 minutes, resulting in mineral loss (demineralization). • Perhaps the single strongest predictor of disease acquisition and progression, is frequency (rather that quantity or source) of fermentable carbohydrates (e.g. sweetened milk, juice, soda). (CALL OUT BOX) • “White Spot lesions” - Clinically, this is the first detectable stage of tooth decay. It is an area of demineralization, characterized by a chalky, white appearance. Although white spot lesions represent loss of mineral from the tooth, the loss is localized mainly in the subsurface of the enamel. The enamel surface in the incipient lesion is essentially intact and amenable to remineralization. THIS STAGE IS REVERSIBLE. • “Cavities” - When demineralization exceeds remineralization as a result of frequent or prolonged acid attacks, the result is a breakdown of the enamel, and the formation of a hole or “cavity” in the tooth surface. This is a late-stage sign of tooth decay. Cavities are not reversible, but can be arrested with intense diet control and oral hygiene and topical application of fluoride.
Early Childhood Tooth Decay Prevalence, acuity and consequence of ECC? • Despite it being easily preventable, ECC continues to be a public health issue. • Dental caries affects approximately 1/5th of preschoolers, ½ of second graders (3, 36) • 80% of tooth decay is concentrated in 25% of children (37) • Low income children, who suffer the most from dental disease, have the least access to care • Call-out box: Low income pre-schoolers are twice as likely to experience caries, twice as likely to experience dental pain, have more than twice the extent of dental disease, and are twice as likely to have insurance coverage because of medicaid, but are only ½ as likely to have a dental visit because of lack of access (CDHP 38) • Dental disease, untreated, results in pain, infection, and may inhibit general growth and development (2)
Early Childhood Tooth Decay What is the classical treatment? • Classical treatment typically involves surgical removal and/or restoration of carious teeth (restorative dentistry). Due to age appropriate inability to tolerate outpatient surgical treatment, coupled with the extent of restorative needs, Maria will be treated under general anesthesia. • In the U.S., the initial cost of treating a child in the operating room for severe caries, exceeds 5 million dollars annually. (39) • Does this mouth look like a success story?
Early Childhood Tooth Decay • Restorative dentistry alone, has had minimal impact on outcomes of children with early childhood tooth decay because it is non-therapeutic in that it doesn’t impact the underlying disease process. Relapse remains high and children frequently require a second general anesthetic. (40-43) • Dental restorations are “prosthetic”, rather than therapeutic, in that they function to replace missing tooth structure. The majority of restorations are not bioactive (the exceptions are glass-ionomer cement restorations that release fluoride). • Early childhood tooth decay is a risk factor for future caries and is a good indicator of future caries experience (42, 44-46). Thus, the initial cost of treatment underestimates the long term cost associated with early child hood tooth decay. • With the knowledge that tooth decay is an infectious and transmissible disease, that it is diet dependent and fluoride mediated, and that restorative dentistry has minimal impact on outcomes, the emerging trend in dentistry focuses on Disease Prevention and Disease Management.
Early Childhood Tooth Decay:Disease Prevention What is Disease Prevention? • True Primary Disease Prevention: prevents disease occurrence by avoiding disease determinants. In tooth decay, this relates to reducing the reservoir of bacteria, reducing transmission and reducing colonization of cariogenic bacteria. (Reservoir vector receptor). • Reducing the reservoir: xylitol chewing gum (use of xylitol containing chewing gum has been shown to inhibit mutans streptococci colonization and reduce the caries experience in children (47, 48) stannous fluoride and chlorhexidine (with dental repair) • Reducing transmission: avoid sharing utensils, cleaning pacifier in mouth etc. • Reducing colonization: oral hygiene (brushing with fluoridated toothpaste), diet control (reduce frequency of carbohydrates) and topical fluoride application (e.g. fluoride varnish)* • What is the role of fluoride? • Antibacterial action on plaque bacteria • Inhibits demineralization • Enhances remineralization
Early Childhood Tooth Decay:Disease Prevention PATHOGENIC FACTORS Cariogenic Bacteria Frequent Carbohydrate Ingestion Reduced Salivary Function PROTECTIVE FACTORS Reduce the Reservoir Dietary Control Fluoride Optimal Oral Hygiene Saliva (Flow/Components) TOOTH DECAY HEALTHY TOOTH
Early Childhood Tooth Decay:Disease Prevention Primary disease prevention may be achieved with early intervention and anticipatory guidance: Anticipatory guidance • In dentistry, this involves informing parents of the conditions that create caries & cavities; its natural progression; and its prevention. Dental Home • The concept of the “dental home” is derived from the AmericanAcademy of Pediatrics concept of the “medical home” (49). It affords the opportunity for prevention. • Goal is to reduce risk of preventable disease • Provides risk assessment; tailored counseling; anticipatory guidance; emergency plan; access to comprehensive dental care, including any necessary referrals Age One Dental Visit • Accepted policy by ADA, Pediatric Dentists, Pediatricians, and Public Health Association • Intended to allow for true primary prevention, establishment of dental home, and ongoing anticipatory guidance (50) • Consists of history, risk assessment, examination, tailored anticipatory guidance, and counseling
Early Childhood Tooth Decay:Disease Prevention Secondary Disease Prevention: prevents disease by maintaining a state of balance between disease and health. • A state of oral health is not absence of activity, but rather a balance of activity. • The teeth are in a constant state of demineralization (loss of mineral) and remineralization (gain of mineral). When demineralization exceeds remineralization, the earliest signs of tooth decay (“white spot”) begin, however, at this point it is reversible. • Remineralization can occur when there is a balance between diet, oral hygiene and fluoride exposure.
Early Childhood Tooth Decay:Disease Management What is Disease Management? • When children have not had the benefit of primary prevention and anticipatory guidance, and caries activity has progressed to the point that there is tooth destruction, the following concepts are employed: • Disease Suppression: this is suppression of the disease (caries activity) before repairing the teeth. It involves intensive diet control to reduce frequency of acid attack on teeth, fluoride applications to increase remineralization and resistance to attack and gross caries excavation to decrease bacterial load. • Disease Arrest: once caries activity has been suppressed, affected teeth will have lost tooth structure (“cavity”) but will be dark or glassy in appearance and will not need to be restored unless it is an issue of function or esthetics. Dark brown/black discoloration: Arrested Disease
TOOTH DECAY Decay Causing Bacteria Carbohydrates Acid Acid Acid Acid Acid Acid Acid Acid Acid Acid Mineral Loss DEMINERALIZATION SUGAR SUGAR TOOTH DECAY
TOOTH DECAY Saliva (Minerals) Fluoride Acid Acid Acid Acid Acid Acid Acid Acid Acid Acid Acid REMINERALIZATION Decreased Carbohydrate Frequency TOOTH REPAIR
Early Childhood Tooth Decay Delaying and Reducing Transmission, Delays and Reduces Tooth Decay: • Studies on controlling infection and colonization of the oral cavity with the primary etiologic agent for early childhood tooth decay (mutans streptococci) have shown promise. • Mother-child couples receiving prenatal counseling on oral health and preventive care (dental cleanings and fluoride applications) every 6 months, had a significant improvement in oral health and a reduction of mutans streptococci during the 4 year study period. • Children enrolled in the study from before birth to 4 years of age, that received preventive treatment had a reduced caries incidence and delayed S. Mutans colonization (51)
Prevention of oral disease, whether it is periodontal disease or tooth decay, will not work if the populations at risk can not access care. • By identifying the barriers to care, specific action steps can be taken to increase oral health awareness and access for high risk populations.
Barriers to Care What are the common barriers to care? • Low socioeconomic status • Lack of community programs (e.g water fluoridation) • Lack of access (no transportation, inability to get time off work, physical disability) • Lack of resources to pay for care/lack of dental insurance • Inadequate public dental insurance programs • Lack of public awareness and understanding of the importance of oral health • Few dentists accept patients on Medicaid due to low re-imbursement rates, abundance of paperwork, and broken appointments
Action Steps • In March 2000, a forum of experts from a variety of disciplines, convened for the Surgeon General’s Workshop on Children and Oral Health to discuss how to address the disparities in oral health and dental care for America’s children. • Eight major recommendations arose from the deliberations, and were presented at the June 2000 Surgeon Generals’ Conference entitled The Face of a Child (52) • The following recommendations can be used as initial action steps to help not only our nation’s children, but other vulnerable populations, to enjoy comprehensive oral health care, so they may enjoy sound, sustainable health. Within the general action steps are action steps specific to Title V - Maternal and Child Health Federal Block Grant Programs. These specific action steps were published by the Association of Maternal and Child Health Programs and may be found in the issue brief, Putting Teeth in Children’s Oral Health Policy and Programs: The State of Children’s Oral Health and the Role of State Title V Programs.
Start early and involve all: Includes establishing a child’s dental home at age one, identifying high-risk children and promoting individualized preventive regimens in both medical and dental practice, developing community-based health coordinators to promote ongoing integration of oral health with general health care, developing day-care accreditation standards on oral health, and addressing the oral health needs of caregivers to promote more widespread attention to oral health. Title V can ensure that the provision and promotion of dental and oral health services are integrated into all aspects of maternal and child health program implementation, needs assessment, policies, and planning, including those affecting children with special health care needs (CSHCN). Oral health status should be incorporated into every prenatal care or public health clinic visit. Action Steps
Assure competencies: Includes developing common core curricula on oral health for all health professionals and developing accreditation standards, guidelines, and performance measures that assure the inclusion of oral health promotion and, where appropriate, treatment in professional training and practice. Title V can assist in training private and public health care practitioners about the oral health needs of children, pregnant women and other vulnerable populations, to ensure that these needs are covered in a comprehensive exam. Title V can utilize its knowledge of training to expand the capacity of private and public sectors, to ensure oral health needs are incorporated into routine primary and preventive care. Action Steps
Be accountable: Includes promoting school-based prevention, education, screening , and referral programs on oral health and developing performance measures and tracking systems to ensure that these programs are effectively implemented. Title V can become involved in the development and/or acceptance of appropriate standards of care as well as more extensive performance measures to monitor what level of dental care children get. Performance measures can be used to assess and evaluate dental health services, for example, what percentage of children enrolled in Medicaid and CHIP actually get dental services, reparative services, or complete care. Action Steps
Take public action: Includes developing activist coalitions that ensure stable-funded, community-based comprehensive health promotion and disease prevention and crafting messages that specifically target providers,policy makers, and the public. Title V can collaborate with oral public health programs, private dental delivery systems, dental schools and associations and others, to raise awareness of oral health needs of children (especially CSHCN), and pregnant women, to ensure access to care and to evaluate existing and new program approaches. Action Steps