Download
1 / 1
10 likes | 142 Views
Ealing Hospital NHS Trust Uncomplicated Miscarriages: To operate or not to operate? Charity Khoo, Aikaterini Iatropoulou, Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom. INTRODUCTION

E N D
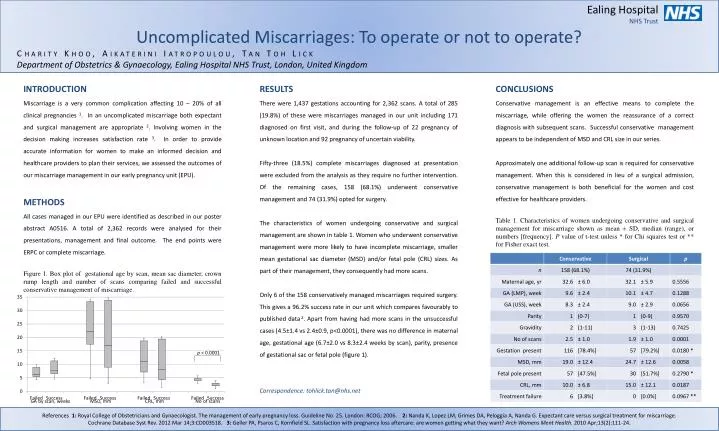
Ealing Hospital NHS Trust Uncomplicated Miscarriages: To operate or not to operate? Charity Khoo, AikateriniIatropoulou, Tan Toh Lick Department of Obstetrics & Gynaecology, Ealing Hospital NHS Trust, London, United Kingdom INTRODUCTION Miscarriage is a very common complication affecting 10 – 20% of all clinical pregnancies 1. In an uncomplicated miscarriage both expectant and surgical management are appropriate 2. Involving women in the decision making increases satisfaction rate 3. In order to provide accurate information for women to make an informed decision and healthcare providers to plan their services, we assessed the outcomes of our miscarriage management in our early pregnancy unit (EPU). METHODS All cases managed in our EPU were identified as described in our poster abstract A0516. A total of 2,362 records were analysed for their presentations, management and final outcome. The end points were ERPC or complete miscarriage. Figure 1. Box plot of gestational age by scan, mean sac diameter, crown rump length and number of scans comparing failed and successful conservative management of miscarriage. GA by scan, weeks MSD, mm CRL, mm No of scans RESULTS There were 1,437 gestations accounting for 2,362 scans. A total of 285 (19.8%) of these were miscarriages managed in our unit including 171 diagnosed on first visit, and during the follow-up of 22 pregnancy of unknown location and 92 pregnancy of uncertain viability. Fifty-three (18.5%) complete miscarriages diagnosed at presentation were excluded from the analysis as they require no further intervention. Of the remaining cases, 158 (68.1%) underwent conservative management and 74 (31.9%) opted for surgery. The characteristics of women undergoing conservative and surgical management are shown in table 1. Women who underwent conservative management were more likely to have incomplete miscarriage, smaller mean gestational sac diameter (MSD) and/or fetal pole (CRL) sizes. As part of their management, they consequently had more scans. Only 6 of the 158 conservatively managed miscarriages required surgery. This gives a 96.2% success rate in our unit which compares favourably to published data 2. Apart from having had more scans in the unsuccessful cases (4.5±1.4 vs 2.4±0.9, p<0.0001), there was no difference in maternal age, gestational age (6.7±2.0 vs 8.3±2.4 weeks by scan), parity, presence of gestational sac or fetal pole (figure 1). Correspondence: tohlick.tan@nhs.net CONCLUSIONS Conservative management is an effective means to complete the miscarriage, while offering the women the reassurance of a correct diagnosis with subsequent scans. Successful conservative management appears to be independent of MSD and CRL size in our series. Approximately one additional follow-up scan is required for conservative management. When this is considered in lieu of a surgical admission, conservative management is both beneficial for the women and cost effective for healthcare providers. Table 1. Characteristics of women undergoing conservative and surgical management for miscarriage shown as mean ± SD, median (range), or numbers [frequency]. P value of t-test unless * for Chi squares test or ** for Fisher exact test. References 1:Royal College of Obstetricians and Gynaecologist. The management of early pregnancy loss. Guideline No. 25. London: RCOG; 2006. 2: Nanda K, Lopez LM, Grimes DA, Peloggia A, Nanda G. Expectant care versus surgical treatment for miscarriage. Cochrane Database Syst Rev. 2012 Mar 14;3:CD003518. 3: Geller PA, Psaros C, Kornfield SL. Satisfaction with pregnancy loss aftercare: are women getting what they want? Arch WomensMent Health. 2010 Apr;13(2):111-24.