Download
1 / 92
920 likes | 956 Views
Explore the pathogenic track to urinary tract infections (UTIs) with an emphasis on definitions, epidemiology, risk factors, etiology, and prevention strategies. Learn about the various types of UTIs, key causative organisms, predisposing factors, complications, and effective treatments. This comprehensive guide will help you grasp the complexities of UTIs and empower you with knowledge to better manage and prevent these common infections. Dive into the world of UTIs to promote urinary health and overall well-being.

E N D
ShadiZiaie Board of clinical pharmacy Assistant professor of SBMU Labbafinejad Hospital Urinary Tract Infection(UTI)
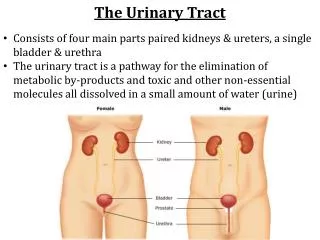
Definition • Significant bacteriuria in presence of symptoms at any level of urinary tract - Bladder: cystitis - Urethra: urethritis - Renal pelvis: pyelitis - Renal parenchyma: pyelonephritis
Urinary Tract Infection • Upper urinary tract Infections • Pyelonephritis • Lower urinary tract infections • Cystitis(traditional UTI) • Urethritis(often sexually-transmitted) • Prostatitis
Epidemiology Worldwide, 150 million cases / year 90 % cystitis 10 % pyelonephritis 75 % sporadic 25 % recurrent 2 % complicated
25-35% of women between ages of 20 - 40 years • 30 times more likely in young women than young men • Incidence after age 65 same in men and women
Prevalence • Almost half of all women will have at least one UTI in their lives. • The risk of UTI in women increases after menopause • After a UTI: 20 - 40 % will have a recurrence • Recurring infections are usually reinfections. • Asymptomatic bacteriuria in women ↑with age & occurs in 2.7% of 15 - 24 year olds 9.3% of over 65 year olds 20 - 50% of over 80 year olds
UTI is rare in young and middle-aged men • Often with catheterisation or urological procedures. • Bacteriuria in elderly men occurs in • 10% of those living at home, • 20% of those living in nursing homes • 30% of those who are in hospitals • Urinary catheter increases the risk almost ten-fold in hospitalised patients and those in other care homes. • Pyelonephritis is common in patients who have been catheterised for over a month.
Infant and children : Male >> female Adolescent-menopause : Female >> male Older age : Female = = male Women: Short ureter Sexual contact : Colonization of pathogens in bladder Spermicidal : Change of normal flora Men (<50) : Prostate infection, anatomical defects , Lack of circumcision, homosexuals
Risk Factors • Obstruction ,congenital, stones • Reflux • Retention • Diabetes Mellitus • Age • Alteration of vaginal flora : antibiotics, spermicide • Insertive rectal intercourse
Predisposing Factors • Prostatic hypertrophy • Urethral strictures • Calculi • Tumors • Bladder diverticula • Anticholinergic drugs • Neurologic malfunctions associated with stroke • Diabetes • Spinal cord injuries • Other neuropathies • Conditions resulting in residual urine volumes:
Complicated or Un-Complicated UTI • UncomplicatedUTI is the one occurring in a healthy young nonpregnant woman. • Complicated UTI is the one occurring in anyone else.
Etiology • Bacteria causing UTIs usually originate from host bowel flora • Virtually every organism associated with UTIs • Certain organisms predominate due to specific virulence factors • Escherichia coli • Most common cause of uncomplicated UTIs • 85% of community-acquired infections
Etiology • Additional causative organisms in uncomplicated infections • Staphylococcus saprophyticus (5% to 15%) • Klebsiella pneumoniae • Proteus spp. • Pseudomonas aeruginosa • Enterococcus spp. (5% to 10%)
Etiology • Other frequently isolated organisms in complicated infections • Proteus spp. • K. pneumoniae • Enterobacter spp. • P. aeruginosa • Staphylococci • Enterococci
Complicated infections • Enterococci • 2nd most frequently isolated organisms in hospitalized patients • May be related to extensive 3rd generation cephalosporin use, not active against enterococci • Vancomycin-resistant Enterococcus faecalis and Enterococcus faecium • Widespread, major therapeutic and infection control issues • Especially long-term hospitalization or underlying malignancy • Susceptible to few antimicrobials
Staphylococcus aureus infections • May arise from urinary tract • More commonly from bacteremia producing metastatic abscesses in the kidney • Candida spp. common cause of UTI in critically ill and chronically catheterized patient • Most UTIs caused by single organism • Multiple organisms isolated in certain patients • Stones, indwelling urinary catheters, chronic renal abscesses • May represent contamination; repeat evaluation
Pathogenesis • Bacterial Invasion • Ascending route 95% • Hematogenous • Lymphatic • Ascending route via the urethra • Men longer urethra/prostatic secretions • Women shorter urethra/colonization • Chance of infection increased by obstruction or foreign body
Pathogenesis • After bacteria enter the urinary tract, infection depends on • Bacteria virulence • Size of inoculum • Host defenses
Host defenses • Bacterial Adherence plays major role in bacteria infectivity • Anti-adherence mechanisms include • Interference by normal bacteria flora • Urinary immunoglobulins • Muco and oligosaccharides may block binding • Mechanical - dilution and flushing • Under normal circumstances, urine inhibits and kills microorganisms • Low pH, osmolality extremes • High urea concentration • High organic acid concentration
Patients unable to void urine completely • Greater risk for UTIs • Recurrent infections common • Even small residual amounts of urine in bladder causes less favorable treatment response • Additional host factors may play role in UTI prevention • Lactobacillus in vaginal flora • Produce lactic acid • Help maintain low vaginal pH preventing vaginal E. coli • Circulating estrogen • Supports vaginal lactobacilli in premenopausal women
Decreases in lactobacilli colonization? • Spermicides • β-lactam antimicrobials • Lower estrogen levels • Intercourse with new partner • Douching
Clinical Presentation • Elderly patients often have nonspecific symptoms • Altered mental status • Change in eating habits • Gastrointestinal symptoms • Patients with indwelling catheters or neurologic disorders commonly do not have lower tract symptoms • May have flank pain and fever • May develop upper tract infections with bacteremia and no/minimal urinary tract symptoms
Urine Collection • Midstream clean-catch method • Preferred for routine collection • Clean urethral opening area • Void and discard 20 to 30 mL • Collect next part of urine flow • Process immediately • Refrigerate as soon as possible • Specimens at room temperature for several hours may have falsely elevated bacterial counts
Urine Collection • Catheterization ? • Uncooperative patients • Patients unable to void urine • Results reliable with careful aseptic technique • May introduce bacteria into bladder • Associated with infection in 1% to 2% of patients
Bacterial Count UTI diagnosis is based on significant numbers of bacteria in urine Historically, bacterial counts equal to or greater than 100,000 organisms/mL of urine in a "clean-catch" specimen were judged to indicate true infection. Counts less than 100,000 organisms/mL of urine, however, may represent true infection in certain situations: with concurrent antibacterial drug administration, rapid urine flow, low urinary pH, or upper tract obstruction.
Pyuria • White blood cell (WBC) count >10 WBC/mm3 of urine • Pyuria in symptomatic patients correlates with significant bacteriuria • Nonspecific • Presence of inflammation • Not necessarily infection • Sterile pyuria associated with urinary tuberculosis, chlamydial, fungal urinary infections
Hematuria and Proteinuria • Hematuria • Microscopic or gross • Common in UTI patients • Nonspecific • May indicate other disorders • Renal calculi • Tumors • Glomerulonephritis • Proteinuria common with infection
Chemistry • Common dipstick test • Detects nitrite formed by nitrate reducing bacteria • False-positives uncommon • False-negatives more common; bacteria do not reduce nitrate • Gram-positive organisms • P. aeruginosa • False test caused by • Low urinary pH • Frequent voiding • Dilute urine
Culture • Most reliable diagnostic method, “gold standard” • Bladder urine normally sterile • Differentiate contamination from infection by quantifying number of bacteria in urine sample • Determine organism susceptibility after identification and quantification • Select agent for treatment • Bacterial susceptibility • Achievable antibiotic urine concentration
Management • Nonspecific therapies in UTI treatment and prevention • Fluid hydration: rapid dilution of bacteria and removal of infected urine by increased voiding • Critical factor: residual volume after voiding • As little as 10 mL of residual urine can significantly alter eradication of infection • Paradoxically, increased diuresis may promote susceptibility to infection by diluting normal antibacterial properties of urine
Large volumes of cranberry juice increase antibacterial activity of urine and prevent UTIs • Fructose and other unknown substances (condensed tannins) interfere with pathogen adherence mechanisms • Urine acidification does not appear to play significant role • Acidifying urine with systemic agents not recommended
Urinary analgesics such as phenazopyridine HCl used by many clinicians • Pain/dysuria are consequence of infection • Urinary analgesics have little clinical role • Most symptoms respond rapidly to antibiotics • Urinary analgesics may mask signs/symptoms of UTIs not responding to antimicrobials
Lactobacillus probiotics • May aid in preventing female UTIs • Lowers vaginal pH which decreases E. coli colonization • Topical estrogen replacement may help prevent recurrent UTIs in postmenopausal women • Decreases vaginal Lactobacillus • Decreases pH and E. coli colonization
Pharmacologic Therapy • Ideal antimicrobial agent • Well tolerated • Well absorbed • High urinary concentrations • Spectrum of activity limited to known or suspected pathogen(s)
Pharmacologic Therapy • Categorize type of infection • Acute uncomplicated cystitis • Symptomatic abacteriuria • Asymptomatic bacteriuria • Complicated UTI • Recurrent infection • Prostatitis • Antibiotic choice based on geographic resistance patterns and patient's recent antibiotic exposure
Acute Uncomplicated Cystitis • Most common form of UTI • typically women of childbearing age • often related to sexual activity • Predominantly E. coli • Other causes: S. saprophyticus, K. pneumoniae, Proteus mirabilis • Many clinicians advocate cost-effective management • urinalysis • empirical therapy without urine culture
Symptomatic Abacteriuria • Symptomatic abacteriuria: acute urethral syndrome • Females present with dysuria and pyuria • Urine culture reveals < 105 bacteria/mL of urine • >50% of dysuria complaints • Most patients with pyuria have infection that requires treatment • Trimethoprim-sulfamethoxazole single-dose or short-course effective • Prolonged courses not necessary for most patients • Obtain culture if single-dose or short-course therapy ineffective
Symptomatic Abacteriuria • Recent sexual activity: consider therapy for C. trachomatis • 1 g azithromycin • Doxycycline 100 mg BID for 7 days • Treatment of sexual partners often required
Asymptomatic Bacteriuria • 2 consecutive urine cultures with > 105 organisms/mL of same organism without urinary symptoms • Most patients elderly or pregnant women • Patients typically respond to treatment; however, relapse and reinfection common • Chronic asymptomatic bacteriuria difficult to eradicate
Asymptomatic Bacteriuria • Management depends on age and whether patient is pregnant • Children • Greater risk of renal scarring/long-standing renal damage • Treat with conventional therapy for symptomatic infection • Greatest risk of renal damage at ages < 5 years
Acute Pyelonephritis • Treat high-grade fever (> 38.3°C) and severe flank pain as acute pyelonephritis • Manage aggressively • Hospitalize severely ill patients • nausea, vomiting, dehydration • IV antimicrobials initially • Milder cases managed outpatient with PO antibiotics
Acute Pyelonephritis • Agents of choice: trimethoprim-sulfamethoxazole, fluoroquinolones • If Gram stain reveals gram-positive cocci, consider Streptococcus faecalis • Direct treatment against this potential pathogen (ampicillin) • Close follow-up mandatory to ensure success
Acute Pyelonephritis • Empirical antibiotic regimens • IV fluoroquinolone • aminoglycoside + ampicillin • extended-spectrum cephalosporins + aminoglycoside • aztreonam • β-lactamase inhibitor combinations • ampicillin-sulbactam, ticarcillin-clavulanate, piperacillin-tazobactam • carbapenems • imipenem, meropenem, ertapenem • IV trimethoprim-sulfamethoxazole
Acute Pyelonephritis • Consider P. aeruginosa, enterococci, multiply resistant organisms if patient hospitalized within past 6 months, urinary catheter, nursing home resident • Treatment recommendations • ceftazidime • ticarcillin-clavulanate • Piperacillin • Aztreonam • Meropenem • Imipenem + aminoglycoside
Acute Pyelonephritis • 3 days aminoglycoside combination therapy followed by nonaminoglycoside single-agent therapy for 7 days: 100% cure rate in experimental animals • Effective therapy should stabilize patient within 12 to 24 hours • significant reduction in urine bacterial concentrations within 48 hours • consider alternative agent based on susceptibility if inadequate bacteriologic response • If patient fails to respond in 3 to 4 days or has persistently positive blood or urine cultures, exclude • bacterial resistance • possible obstruction • papillary necrosis • intrarenal or perinephric abscess • other disease process
UTIs in Males • Often more difficult to manage than in females • Incidence of infection in males < 60 years much less than in females • Infection related to urinary tract manipulation • urinary tract instrumentation • catheterization • renal and urinary stones • Conventional view: males require prolonged treatment • Obtain urine culture before treatment • Cause not as predictable as in women