Download
1 / 75
930 likes | 1.57k Views
PANCREAS. JR. BASIC SCIENCE. ANATOMY & PHYSIOLOGY. ANATOMY : -Retroperitoneal -Regions: * Head : Adjacent to C-loop and posterior to transverse mesocolon, anterior to vena cava, right renal artery, and renal veins. CBD transverses the

E N D
PANCREAS JR. BASIC SCIENCE
ANATOMY & PHYSIOLOGY
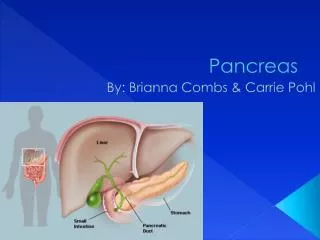
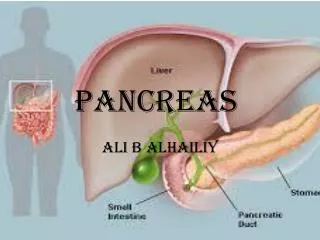
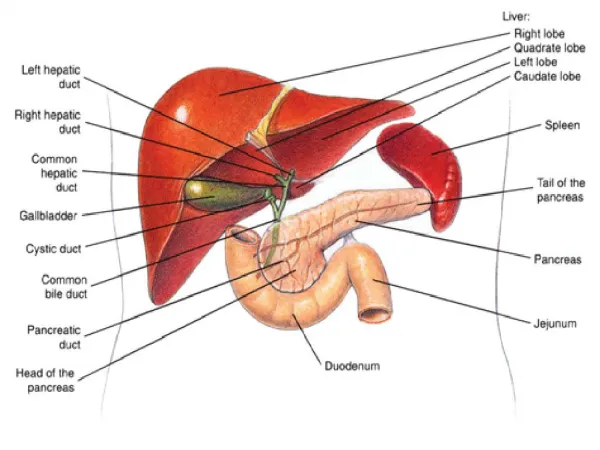
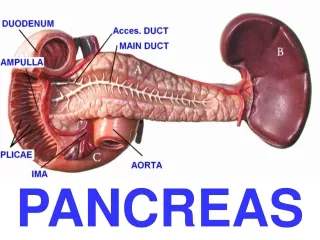
ANATOMY: -Retroperitoneal -Regions: *Head: Adjacent to C-loop and posterior to transverse mesocolon, anterior to vena cava, right renal artery, and renal veins. CBD transverses the pancreatic head and joins the main pancreatic duct at the ampulla of Vater *Neck: Anterior to portal vein *Uncinate process: Wraps around portal vein and ends posteriorly in the space between the SMA and SMV *Body & Tail: Anterior to splenic artery and vein. Located in floor of lesser sac posterior to stomach. Covered by gastrocolic omentum.
Embryology: -The pancreas forms from two diverticulae of the endodermal lining of the foregut in a region which later becomes the duodenum. -The dorsal pancreatic bud passes anterior to the portal vein (forms head,neck, body, & tail). -The ventral pancreatic bud is smaller and rotates around behind the duodenum (forms caudate part of the head & the uncinate process. -Both buds then usually fuse (~8 weeks). -Ducts develop in both buds and fuse. -Pancreatic duct is usually 2-3 mm in diameter.
-Duct of Wirsung starts at the tail and extends to the head. It terminates at the papilla of Vater. It is derived from the ventral pancreatic bud. -Duct of Santorini (accessory pancreatic duct) drains a small upper portion of the pancreatic head and terminates in the duodenum as a small accessory papilla. It is derived from the dorsal pancreatic bud.
PANCREAS DIVISUM: -In 10% of patients, the ducts of Wirsung and Santorini fail to fuse. -Most of the pancreas is then drained through the duct of Santorini and the minor papilla. -In some of these patients, the minor papilla is unable to handle the volume of pancreatic juices produced by the gland, resulting in a relative outflow obstruction. -Can result in pancreatitis. -Treatment: Sphincteroplasty of minor papilla.
SPHINCTER OF ODDI: -The main pancreatic duct joins with the common bile duct and empties into the ampulla of vater in the second portion of the duodenum. -Muscle fibers around the ampulla form the Sphincter of Oddi. -Contraction and relaxation of the Sphincter of Oddi are regulated by hormones and neuronal control.
ARTERIAL SUPPLY: • -Celiac axis gives off common hepatic, which gives rise • to GDA, which becomes superior pancreaticoduodenal • artery as it passes behind the 1st portion of the • duodenum. This branches into the anterior and • posterior superior pancreaticoduodenal arteries. • -The SMA gives off the inferior pancreaticoduodenal • artery as it passes behind the neck of the pancreas. • This divides into the anterior and posterior inferior • pancreaticoduodenal arteries. • The superior and inferior pancreaticoduodenal arteries join together to form an arcade of blood vessels supplying the pancreatic parenchyma and duodenum. • The dorsal, great, and pancreatic arteries form connections between the splenic artery and the inferior pancreaticoduodenal artery.
-Venous drainage tends to follow arterial supply. -Lymphatic drainage is diffuse and widespread. Lymphatics connect with the lymph nodes draining the jejunum and transverse mesocolon. There are also lymph nodes adjacent to the head of the pancreas as well as the hilum of the spleen. ***The extensive lymphatics explain why pancreatic cancer often presents with positive lymph nodes and a high incidence of recurrence after resection.***
NEURAL CONTROL OF PANCREATIC SECRETIONS: -Parasympathetics: Stimulate secretion of endocrine & exocrine pancreas. -Sympathetics: Inhibit secreation. -Rich supply of afferent sensory fibers, which are responsible for intense pain associated with pancreatitis and pancreatic cancer.
EXOCRINE PANCREAS: -Secretes 500-800cc/day -Acinar cells contain zymogen granules, which fuse with the membrane and secrete a variety of enzymes into a ductal system -These enzymes are responsible for digestion of food.
ENZYMES: *Amylase: Only pancreatic enzyme secreted in its active form Hydrolyzes starch and glycogen *Gastric hydrolysis of proteins causes peptides to enter the small intestine and release cholecystokinin and secretin, which stimulate the pancreas to release enzymes and bicarbonate. Cl- secretion is inversely related to bicarbonate secretion. *The enzymes are secreted as proenzymes, which are then activated by enterokinase, located in the small intestine. This explains why autodigestion of the pancreas does not occur.
ENDOCRINE PANCREAS: * ~1 million islets of Langerhans (spherical collections of cells scattered throughout the pancreatic parenchyma) * Contain a variety of cells, which secrete a variety of hormones into the bloodstream
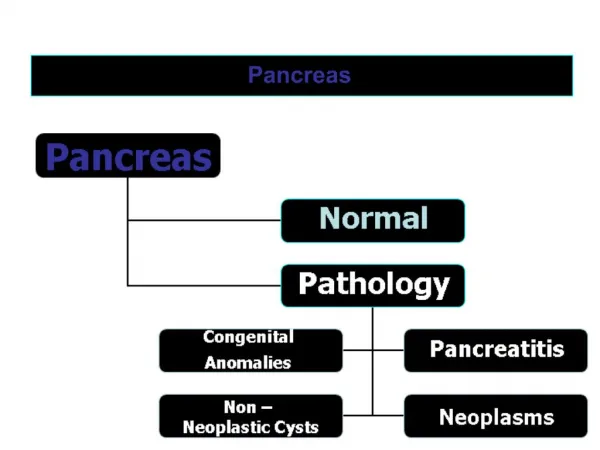
ACUTE PANCREATITIS: *Inflammation of the pancreas with little or no fibrosis of the gland *Due to: Alcohol Biliary tract disease Vasculitis Hyperlipidemia Pancreatic duct obstruction Heredity Neoplasms Hypercalcemia Pancreas divisum Trauma Ampullary and duodenal lesions Surgical Infections ERCP Venom (scorpion) Ischemia Drugs (thiazides, lasix, estrogens, Hypoperfusion azathioprine, methyldopa, 6-MP, etc) Embolic Idiopathic
BILIARY TRACT DISEASE: Colocalization Theory:
ALCOHOL: -Pancreatitis may occur after a single use, but more often occurs in patients who have used 100-150g/day of alcohol >2 years. (10-15%) -Can be recurrent after continued alcohol abuse. -Mechanism: *Ethanol causes sphincter of Oddi spasm. (Blockage) *Ethanol is a metabolic toxin to pancreatic acinar cells, which interferes with enzyme synthesis and secretion. *Get initial secretory increase followed by inhibition. Enzymes and calcium precipitate within the pancreatic duct, resulting in multiple obstructions. *Ethanol increases ductal permeability. Enzymes leak out into surrounding tissue. *Ethanol transiently decreases pancreatic blood flow, causing focal ischemia.
Pathophysiology of acute pancreatitis: ***Ultimate severity of pancreatitis depends on the extent of the systemic inflammatory response and cytokines that play a role in activation and migration of inflammatory cells.***
DIAGNOSIS: *Diagnosis of exclusion—Rule out perforated peptic ulcer, gangrenous small bowel obstruction, and cholecystitis. (Require immediate intervention) -Abdominal pain (usually epigastric), usually after a meal. -”Knifing” or “boring” pain through to the back—relieved by leaning forward. -Nausea and vomiting, with continued retching after stomach is emptied. Vomiting does not relieve the pain. -Tachycardia, tachypnea, hypotension, fever -Voluntary/Involuntary guarding -Decreased or absent bowel sounds -Abdomen may be distended with intraperitoneal fluid -Blood from necrotizing pancreatitis dissects through soft tissues and causes a bluish discoloration around the umbilicus (Cullen’s sign) or flanks (Gray Turner sign)
Serum amylase: -usually increases immediately with onset of pancreatitis & peaks within a few hours (However, may be normal in pancreatitis) -remains elevated 3-5 days -no correlation between magnitude of elevation & severity of pancreatitis -can also be elevated with SBO, perforated duodenal ulcer, other intra-abdominal inflammatory conditions Urine amylase: -may be more sensitive than serum amylase in detection of pancreatitis (lipids may interfere with measurement of serum amylase) -levels remain elevated for several days longer than serum amylase Pancreatic-specific amylase: -More specific for pancreatitis (88-93%) Serum lipase: -Remains elevated longer than serum amylase.
Imaging: *CT: uniform enhancement of pancreas *Ultrasound
RANSEN’S CRITERIA Prognosis: <2: Mortality-0 3-5: Mortality 10-20% >7: Mortality >50% *Only useful for 1st 48h APACHE II score: (acute physiology & chronic health evalutation) -uses vital signs, labs, age, and chronic health status of patient - >8 is severe
TREATMENT: *Mild pancreatitis: (no systemic complications, low Ranson’s & Apache II score) -IVF resuscitation/maintenance -Pain management (avoid morphine due to Sphicter of Oddi contraction) -Supportive (rest the pancreas) -NPO -NGT -H2 blockers *No abx unless suspect infection -Slow feeding after pain subsides, amylase decreases, patient feels hungry
Severe Pancreatitis: (Ranson’s >7, Apache II >8, systemic symptoms) -ICU & Supportive Care -TPN vs jejunal feeds -If necrotizing: Flagyl, Imipenim, 3rd gen cephalosporin, Diflucan prophylaxis -If necrotizing & septic: Consider necrosectomy
Biliary Pancreatitis: -Treatment controversial -Cholecystectomy once pancreatitis improves before discharge home -If patient still has pancreatitis, but CBD is obstructed, ERCP with sphincterotomy & stone extraction is indicated -Routine ERCP is not indicated due to risk of post-ERCP pancreatitis
-Pain: Midepigastric RUQ or LUQ Penetrating through to the back Steady & boring (not colicky) Often exacerbated by eating & drinking -Pain causes patient to lay still -Nausea/Vomiting -Anorexia, malabsorption, weight loss -Diarrhea/Steatorrhea due to pancreatic exocrine dysfunction -Diabetes due to pancreatic endocrine insufficiency
CHRONIC PANCREATITIS: Incurable, chronic, inflammatory condition -Associated with ETOH in 70% of cases Multiple hit theory: Multiple episodes of acute pancreatitis cause inflammatory changes that result in chronic inflammation & scarring
Histology: Induration, nodular scarring, fibrosis, mononuclear cell infiltrates, patchy areas of necrosis, reduced islet size and number (Sheets of fibrosis & loss of acinar tissue) (Mononuclear cell infiltrate)
Tests for Chronic Pancreatitis: ***Mostly a clinical diagnosis!***
Dilated pancreatic duct with intraductal stones & parenchymal calcification EUS, MRCP, ERCP, transabdominal US
Treatment: -Analgesics, celiac plexus block -Cessation of ETOH -Oral enzyme therapy -Selective use of antisecretory therapy (Octreotide) -Some benefit from ERCP with sphincterotoy/stenting (proximal panc duct stenosis) -Surgery
TRANSDUODENAL SPHINCTEROPLASTY: -Incision of the ampullary, bile duct, & pancreatic duct sphincters -Suture apposition of mucosal edges of the incision -Used for obstruction & inflammation isolated to this region
Puestow: (Lateral pancreaticojejunostomy) -Permits extensive drainage of the pancreatic duct -Drainage procedure for “chain of lakes” (segmental narrowings & dilations of the duct) -Good for pancreatic duct >6mm
Distal pancreatectomy: -Good for inflammatory changes isolated to body & tail -Good for patients without ductal dilation -Leaves pancreas behind– high rate of recurrence
Frey Procedure: Resection of the pancreatic head with longitudinal pancreaticojejunostomy (provides complete decompression of the entire ductal system)
Islet Cell Autotransplantation: -Used to prevent diabetes in pancreatic resection -Need 2-3 million islet cells -Islets are infused into the portal venous system for intrahepatic grafting -Limited by ability to harvest enough islet cells from a sclerotic gland
Complications of chronic pancreatitis: -Pseudocyst: Chronic collection of pancreatic fluid surrounded by a nonepithelialized wall of granulation tissue & fibrosis
-Acute pseudocyst (acute fluid collection): Usually due to pancreatic duct leak with extravasation of pancreatic juice. -Wall of granulation tissue without fibrosis forms around the fluid collection after 3-4 weeks & seals it -50% resolve spontaneously (usually those <6cm)
Treatment: If asymptomatic: expectant -If symptomatic or enlarging: ERCP with stent, cystenterostomy (endoscopically, laparoscopically, or open) -Infected: aspirate/drain ***ANY PSEUDOCYST WITHOUT PRECEEDING ACUTE PANCREATITIS NEEDS INVESTIGATION TO DETERMINE THE ETIOLOGY***
Pancreatic abscess: Pseudocysts that become secondarily infected -Can lead to venous thrombosis, pseudoaneurysms, or hemorrhage
Other complications: -Splenic/portal vein thrombosis (can get gastric varices). Tx: splenectomy -Pancreatic ascites/effusion. Tx: octreotide, bowel rest, TPN -Pancreatic-enteric fistula -Inflammatory mass in head of pancreas
NEOPLASMS OF THE ENDOCRINE PANCREAS
INSULINOMA: • -Most common type of islet cell tumor • -Arise from pancreatic beta cells • -Most common cause of fasting hypoglycemia in adults • -83-92% are single, 8-17% are multiple (MEN) • -84% benign, 16% malignant (metastatic) • -90% sporadic, 10% associated with MEN I • -Physiology: • Tumor secretes excessive insulin • Results in hypoglycemia • The brain reacts with initial excitation (convulsion) • Eventually results in neurologic depression (coma)
Signs/Symptoms (often due to the release of epinephrine as a response to hypoglycemia) Loss of consciousness Tremor Confusion Hunger Weakness/Fatigue Positive Babinski sign Deep coma Paresthesias Sweating Irritability Drowsiness/stupor Transient hemiplegia Lightheadedness Abdominal pain Visual disturbances Palpitations Amnesia Clonic convulsions Headache ***It is not possible to differentiate benign from malignant lesions based on symptoms. ***It is not possible to correlate the size of the tumor with the extent of symptoms.
Diagnosis: • Check insulin to glucose ratio while patient is having symptoms. • -Low glucose, but elevated insulin • Check C-Peptide levels (to rule out exogenous insulin) • -elevated • 3. Check Urine sulfonylureas